Astrocytoma
Findings:
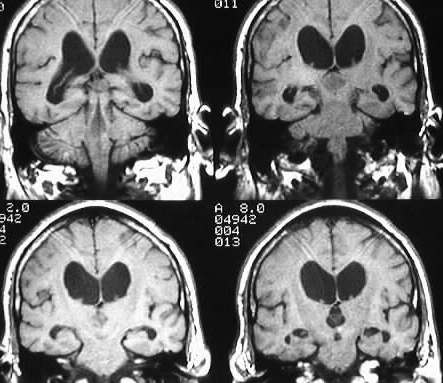
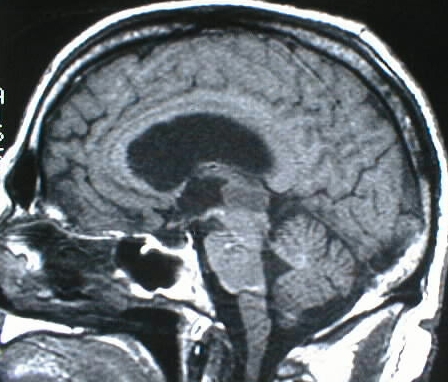
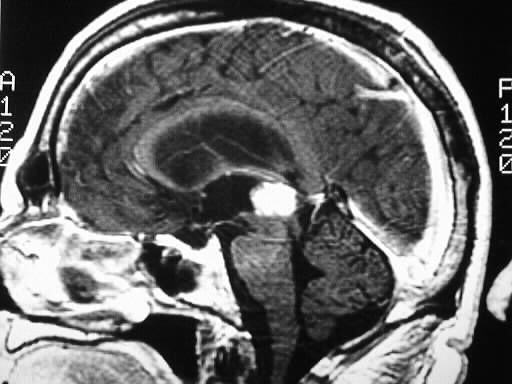
An exophytic, strongly enhancing intraaxial mass is present
in the brainstem at the level of the midbrain, projecting into the posterior
third ventricle, which causes obstructive hydrocephalus by compression
and/or invasion of the cerebral aqueduct.
Differential Diagnosis:
choroid plexus papilloma, ependymoma, intraventricular
meningioma, pineal region tumor (germ cell, pineoblastoma, pineocytoma),
astrocytoma (no distinguishing features in this particular case).
Discussion:
1993 WHO classification:
grade I
-JPA, PXA, SGCA, ganglioglioma, meningioma
grade II
-diffuse astrocytoma, HPC
grade III
-anaplastic astro, HPC
grade IV
-GBM
astrocytoma
-70% of all gliomas
-low grade: children and adults 20-40, no
necrosis or neovascularity, cystic, calcification 20%, fysr 33%
-high grade:>40, necrosis, neovascularity,
hemorrhage. median srv 8 mos.
-spread- natural passages, subpial, subependymal,
WM tracts, may cross meninges
-GBM may be better circumscribed microscopically
than lower grade astro
-necrosis separates GBM from anaplastic
astro
GBM
-most common glioma, peak 45-55yrs., M>F,
10% 2ysr
-deep frontal white matter most common,
temporal lobe and basal ganglia
-expansile, necrosis, ring enhancement,
edema, +/- flow voids
-well circumscribed gross appearance with
wide invasion microscopically
-T2 hyperintensity in corpus callosum =
tumor spread, not edema
BACK TO
MAIN PAGE