
Herpes Encephalitis
(not all same patient)
Findings:
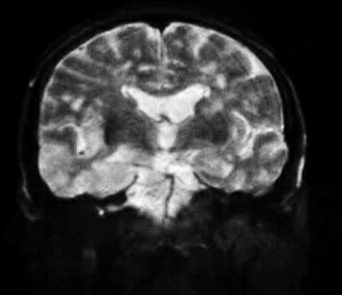
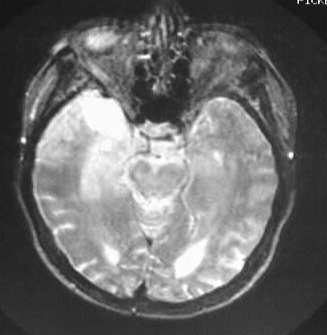
The MR images were obtained on an adult patient, showing
asymmetric abnormal signal in both temporal lobes, extending to the insular
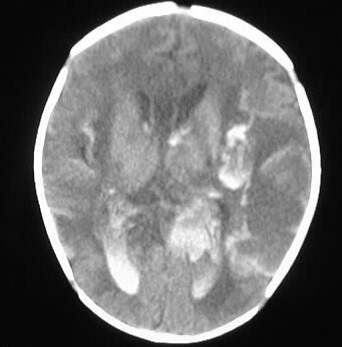
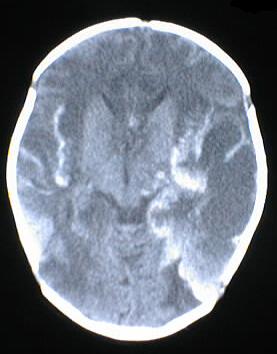
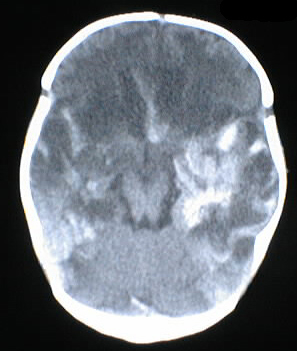
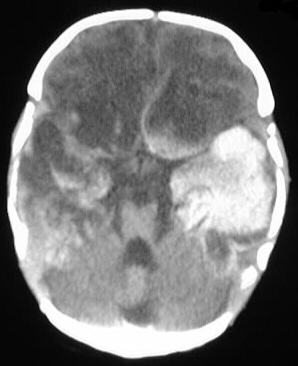
cortex. The CT images are from a pediatric patient, showing extensive hemorrhagic
necrotic changes throughout both cerebral hemispheres with sparing of the
cerebellum. Intraventricular hemorrhage is present as well. The hemorrhagic
process is centered in the temporal lobes.
Differential Diagnosis:
Signal abnormality involving both temporal lobes has
a relatively limited differential diagnosis and is nearly pathognomonic
for herpes encephalitis. Trauma with multifocal contusions and shear injury
could be considered if there was appropriate history. Other less likely
considerations include metastatic disease or multiple venous infarctions.
Discussion:
-most common nonepidemic viral encephalitis
neonatal:
-birth canal transmission- HSV II, usually spontaneous Ab
-attacks endothelium
-2-4 wks-->seizures and severe hemorrhagic encephalitis (no preference for
temporal lobes)
-complications: mental retardation, ventmegaly, microcephaly/microphthalmia,
multicystic encephalomalacia, Ca++
adult, pediatric:
-HSV I reactivation
-prodrome: fever malaise 60%, URI 30%
-seizures, confusion, encephalitis, focal deficits, cranial neuritis, 70%
untreated mortality
-EEG spike and slow wave
imaging:
-50% normal early CT +/- patchy WM/cortical hypo/hyperdensities sparing
BG, thal, cerebellum
-progression to necrosis +/- hemorrhagic, calcification, encephalomalacia
-MR more sensitive for early changes- gray matter edema, possible meningeal
enhancement
-predilection for temporal lobes- latency in trigeminal ganglion, possibly
more P-O involvement in children
-look for cingulate gyrus, insular cortex involvement