

Mycotic Aneurysm
Findings:
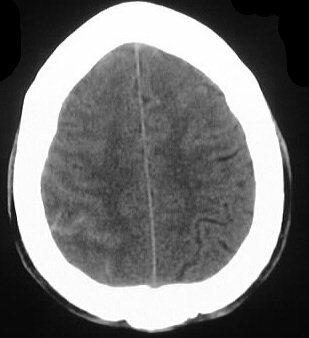
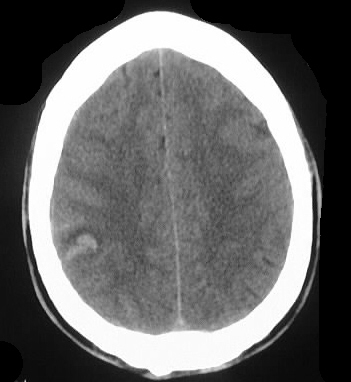
Axial noncontrast CT shows focal hyperdensity in the
right parietal cortex, associated with a small amount of subarachnoid hemorrhage.
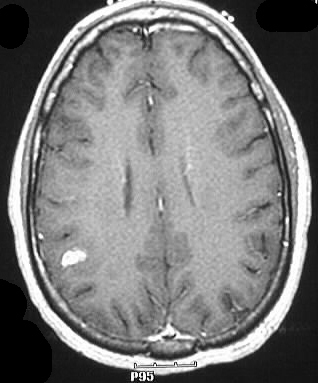
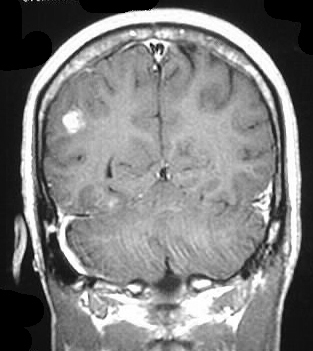
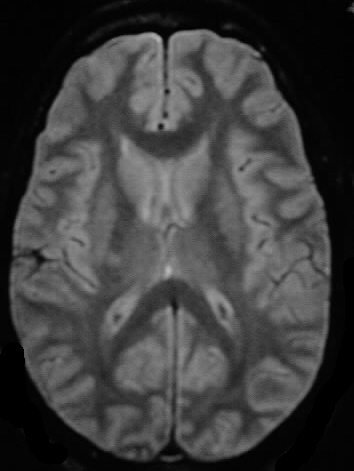
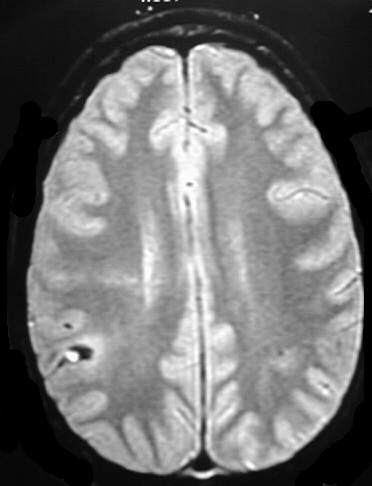
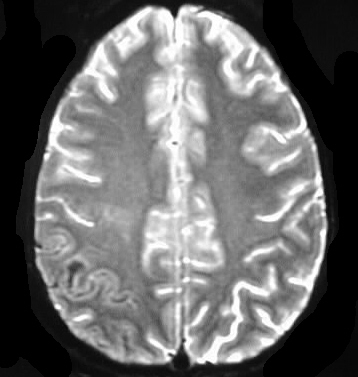
MR images show a focal area of signal abnormality in this same region,
with hyperintensity/enhancement on T1 and hypointensity on T2 consistent
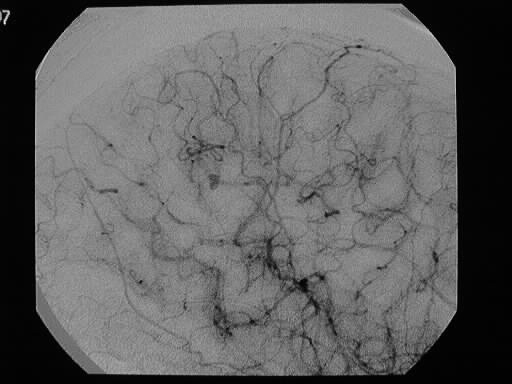
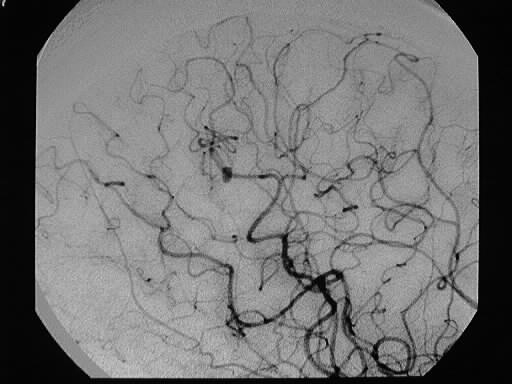
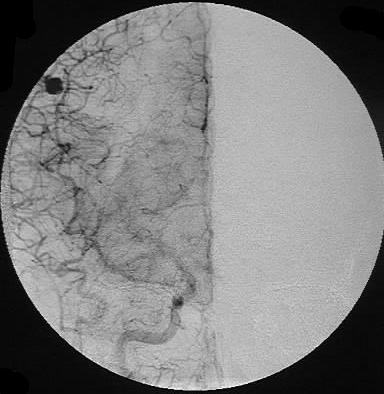
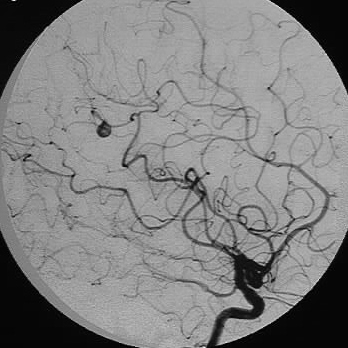
with blood products (intracelular methemoglobin). Cerebral arteriogram
shows a small peripheral aneurysm, which has enlarged somewhat on follow
up angiography (last two images).
Differential Diagnosis:
The differential diagnosis of a small peripheral hemorrhagic
lesion is broad, including trauma, tumor, aneurysm and vascular malformation.
Peripheral aneurysms due to atherosclerosis or underlying congenital vascular
abnormality are very unusual. Etiologies such as mycotic or oncotic aneurysms
should be considered in this location.
Discussion:
Septic emboli from endocarditis may cause brain abscess,
mycotic aneurysm, or vasculitis. Septicemia from any cause may lead to
endocarditis, but the most common is S. aureus endocarditis in IV drug
abusers. Mycotic aneurysms comprise less than 5% of all intracranial aneurysms,
and may be multiple in 20%. The aneurysms are commonly located superficially
over the convexities. These lesions may respond to antibiotics, but may
enlarge on follow up examination and require surgery. Oncotic aneurysm
is a similar process caused by embolization of atrial myxoma tissue. Mycotic
aneurysms have a higher risk of rupture than congential aneurysms.