


Venous angioma with parenchymal hemorrhage and infarction
Findings:
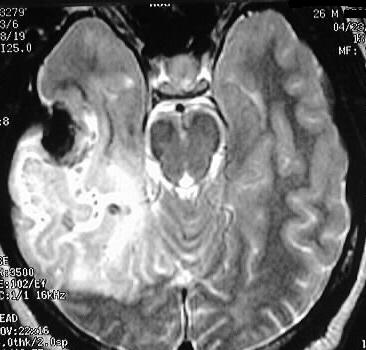
Axial T1 and T2 weighted images show a parenchymal hematoma
in the right temporal lobe, with signal characteristics of acute hemorrhage
(deoxyhemoglobin). A large area of signal abnomality is present in the
right temporoparietal region, consistent with edema and/or ischemia/infarction.
The postcontrast T1 weighted images at a slightly higher level show a large
transcortical draining vein in the right temporal region, associated with
numerous spokelike tributaries.
Differential Diagnosis:
A parenchymal hemorrhage could have numerous etiologies.
In a 26 year old male such as this, trauma, vascular lesion (aneurysm,
AVM, cavernoma/venous angioma), and tumor would be the most common causes.
In this case, the hemorrhage may have been due to an occult cavernoma which
is commonly associated with venous angiomas.
Discussion:
Venous angiomas, also known as developmental venous anomalies,
are the most common vascular malformation of the brain and are seen in
1-2 % of pts studied with contrast MR. 65% are supratentorial, and are
most commonly seen adjacent to the frontal horn of the lateral ventricle.
The lesions represent a stellate venous complex that drains to ventricular
or cortical surface. Since these lesions drain and course through normal
brain, anything that interferes with this drainage can cause infarction
of that territory. Venous angiomas are also associated with cavernomas,
and the hemorrhage uncommonly seen with these lesions may be related to
the cavernoma rather than the venous angioma itself. Alternatively, thrombosis
of the venous angioma can cause hemorrhagic venous infarction. Other associations
include Gorlin's syndrome, heterotopias, schizencephaly, and sinus pericranii.
Venous angiomas are usually an incidental finding. For further discussion
and presentation of cavernomas, please refer to unknown cases #31 and 73.