
Lymphoma
Findings:
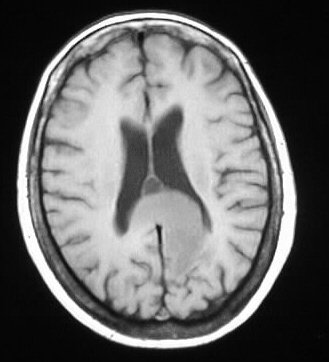
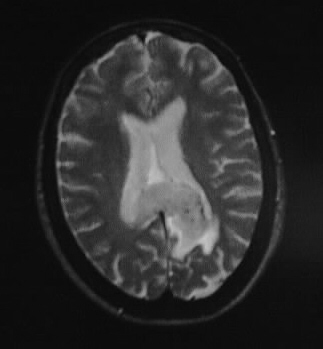
A homogenously enhancing mass crosses and expands the
corpus callosum, originating in the left temporoparietal region. The tumor
shows mildly decreased intensity with respect to the surrounding edema,
indicating a cellular lesion.
Differential Diagnosis:
Lesions that cross the corpus callosum have a relatively
limited differential, including GBM, lymphoma, and possibly tumefactive
MS. The signal characteristics and enhancement are most characteristic
of primary CNS lymphoma.
Discussion:
CNS lymphoma represents up to 15% of primary brain tumors,
with the incidence now equal to meningioma and low grade astrocytoma. Histologically,
these are B-cell tumors. A solidly enhancing mass is more common in immunocompetent
individuals, with necrotic tumors seen in AIDS/immunosuppressed. CNS lymphoma
is an AIDS defining illness in those who are HIV(+), and develops in approximately
2% of AIDS patients. This is the most common CNS mass in pediatric AIDS.
Primary lymphoma is more common than secondary, and up to 50% are multiple.
50% may recur at initial site of origin. Prognosis is 3 months untreated
immunocompetent, 45 days immunocompromised. Average survival is approximately
4 years in treated immunocompetent individuals.
Imaging features/locations:
-well demarcated, periventricular, supratentorial
(85%)
-little edema. rare calcification or hemorrhage
-deep gray 33%, cerebral WM 55%, cerebellum
10%
-common subependymal and perivascular spread
-primary- parenchymal, secondary- dural
(usually)
-hyperdense noncon CT, T2 hypointense
-other ddx- focal cerebritis, mets, GBM,
TB/sarcoid, MS