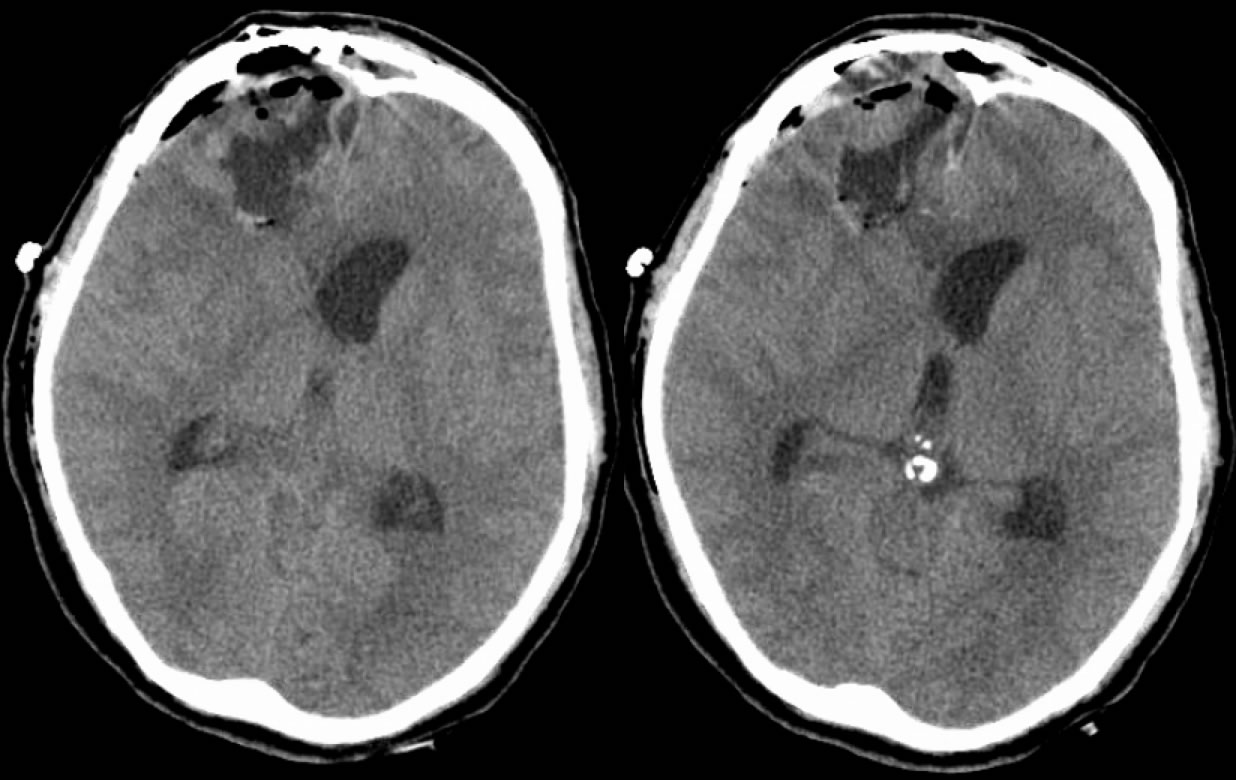
16 hours later, s/p abscess drainage (Pt. is now moribund and expired within 10 hours):
Brain Abscess, complicated by acute ventriculitis
Findings:
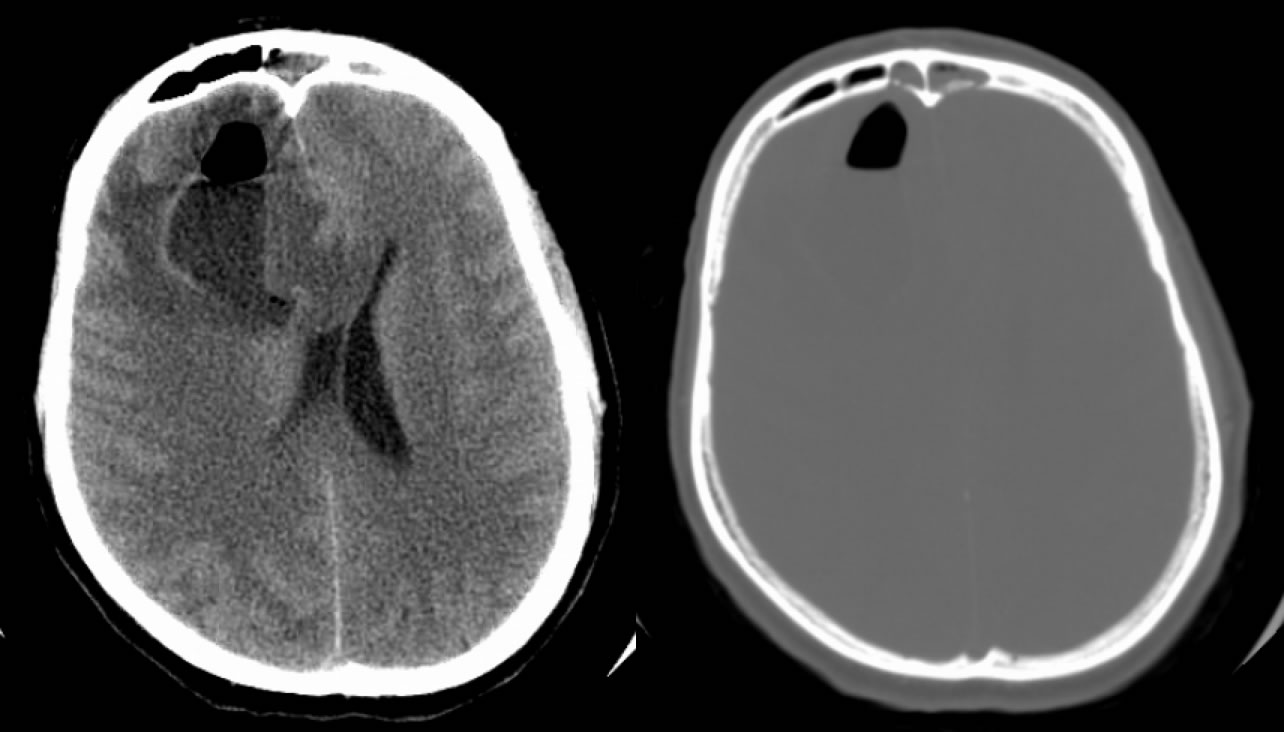
1. Axial noncontrast head CT demonstrates an abnormal fluid collection in the right frontal lobe with an air fluid level and surrounding vasogenic edema, associated with moderate mass effect and ventricular effacement. Bone windows show erosion of the frontal sinus inner table with inflammatory opacification of the frontal sinuses.
2. The short term follow up scan obtained after emergent surgical drainage of the abscess demonstrates a complex fluid/fluid level in the left occipital horn, associated with acute hydrocephalus. There is also hazy complex material within the third ventricle. A complex hemorrhagic right frontal surgical cavity is now present. The findings are compatible with rupture of the abscess with intraventricular pus. This event is usually fatal.
Differential diagnosis:
Brain abscess, necrotic neoplasm (AFL not seen), trauma with contusion and pneumocephalus (unlikely).
Discussion:
-early cerebritis (3-5d), late cerebritis (2 wks), early capsule (>2 wks), late capsule (wks-mos)
-only 50% have fever or WBC count, 90% have headache, most have high ESR
-less than 2.5 cm may be treated with Abx alone, greater need drainage
-internal DWI hyperintensity characteristic, some help in dist GBM/mets from abscess, not absolute
-DWI may be helpful in f/u, development of hyper DWI may indicate recurrence
-T2 hypointense rim with late cerebritis and early capsule, also not absolute
-abscess complications include choroid plexitis, intraventricular rupture with ventriculitis, leptomeningitis/ependymitis, and daughter abscesses
BACK TO
MAIN PAGE