Astrocytoma
Findings:
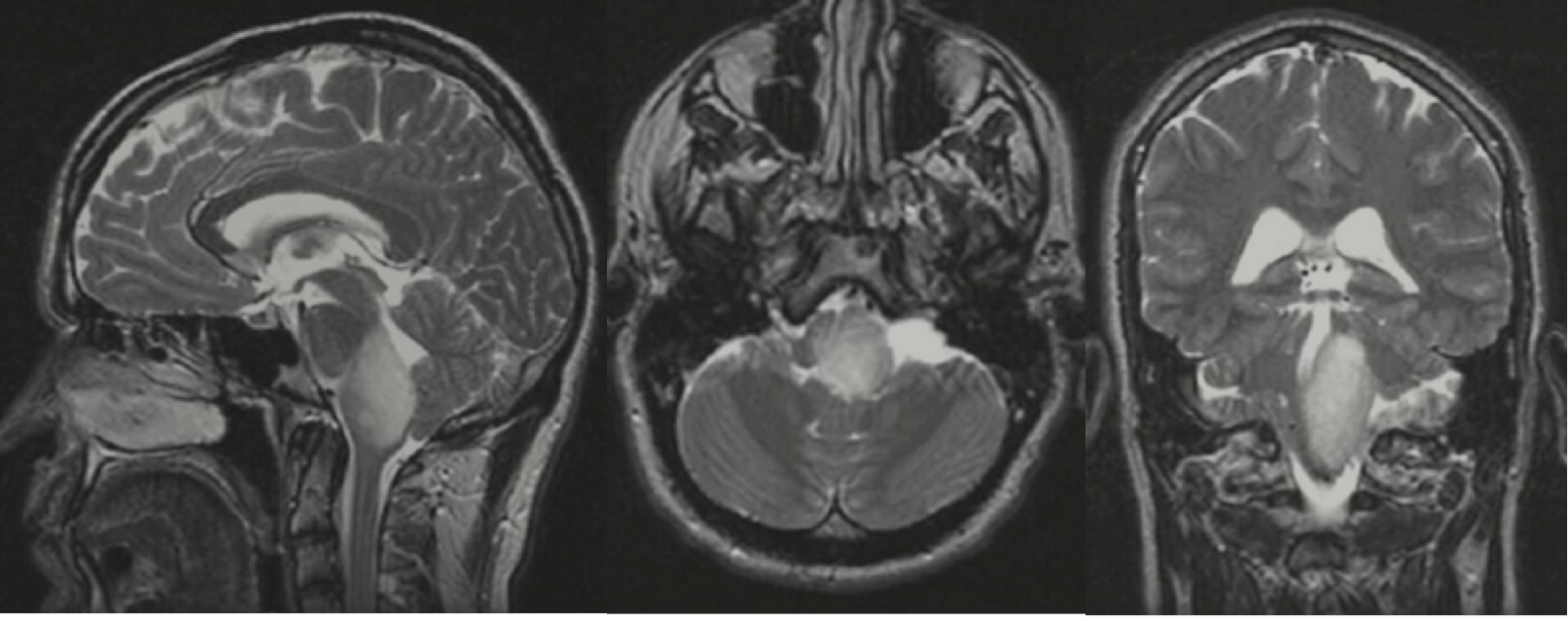
T2WI demonstrates a homogenous hyperintense expansile mass originating from the left medulla. There is adjacent compression of the fourth ventricle and inferior cerebellum.
Differential Diagnosis:
Astrocytoma, unusual encephalitis, hamartoma, infarction.
Discussion:
Astrocytomas are well-differentiated primary brain tumors of astrocytic origin that demonstrate a slow, but infiltrating growth pattern. On CT, WHO diffuse grade 2 astrocytomas appear as ill-defined homogenous hypo/isodense masses that do not enhance. MRI of the lesion will demonstrate a homogenous hypointense mass on T1WI and hyperintense mass of T2WI that may be expansile. Diffuse astrocytomas (WHO grade II) may appear circumscribed and do not enhance. Higher grade astrocytomas may show variable enhancement with ring enhancement and central necrosis concerning for WHO grade 4 gliobastoma multiforme. It is important to note that astrocytomas may appear circumscribed on imaging, but the lesion will often extend beyond the imaged signal abnormality. Two-thirds of astrocytomas occur supratentorial with increased prevalence in the frontal and temporal lobes with relative sparing of the occipital lobe. One-third of astrocytomas occur infratnetorial in the pons and medulla. Infratentorial lesions tend to occur in children and adolescents, although the majority of astrocytomas occur between the ages of 20-45 years. Low-grade astrocytomas have a tendency toward malignant conversion to anaplastic astrocytoma. Due to the inherent tendency toward malignancy, the median survival is 6-10 years.
BACK TO
MAIN PAGE