Chordoma
Findings:
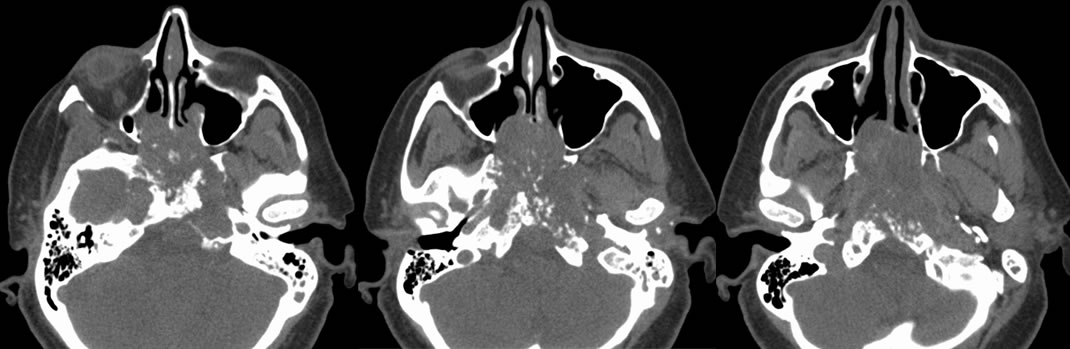
Axial CT images demonstrate a destructive skull base mass that has extended into the posterior nasal and oropharyngeal cavities and involves the sphenoid sinuses. The mass appears calcified secondary to local bone destruction. There is left sided mastoid air cell disease likely related to obstruction of the left eustachian tube.
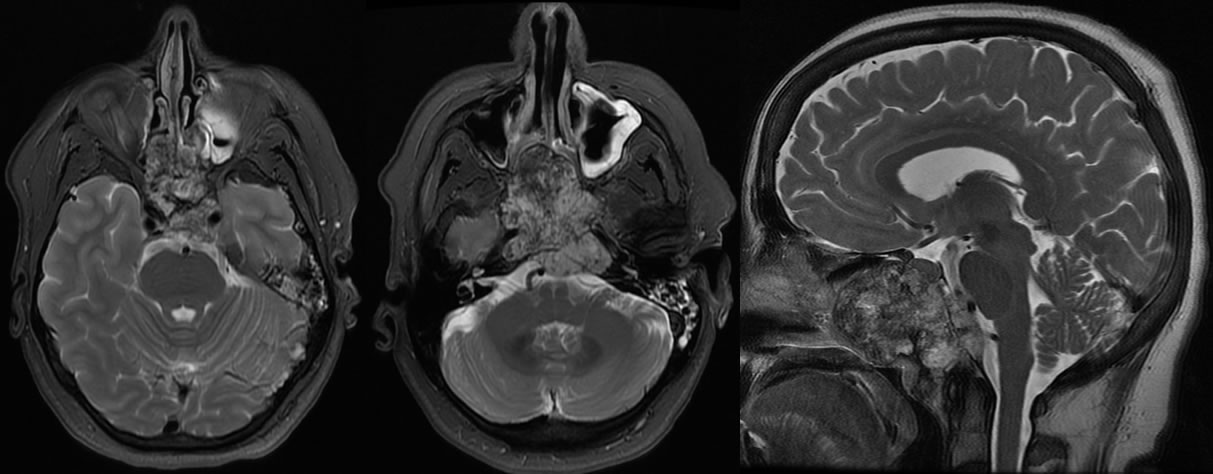
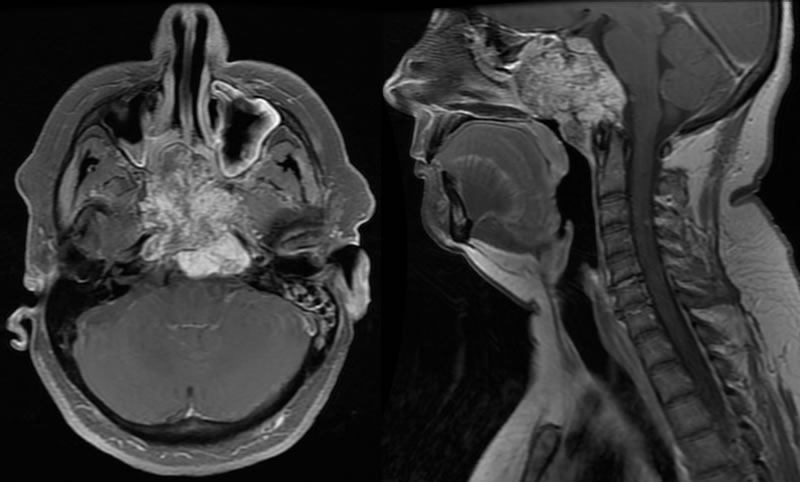
Axial and sagittal T2 images show a heterogenous, multiseptated mass with areas of patchy decreased signal in the anterior aspect of the lesion. Post-contrast T1 images shows that the mass has diffuse patchy irregular enhancement and involves the central skull base and causes occlusion of the nasopharynx. The mass extends through the clivus into the prepontine and premedullary cisterns.
Differential Diagnosis:
Chordoma, chondrosarcoma, metastatic disease
Discussion:
Chordomas are a type of rare, slow growing malignant tumor thought to arise from the remnants of the notochord. They account for 1% of intracranial tumors and 4% of primary bone tumors. Because they arise from remnants of the notocord, they may develop anywhere along the spine. However, the two most common locations are cranially at the clivus and in the sacrum. Chordomas usually present in adults between the third and sixth decades of life and are more common in Caucasians. They are locally invasive, evidenced by the significant local bone destruction in this patient, but rarely metastasize. Typical imaging shows a well circumscribed, centrally located, soft tissue lytic lesion on CT. MR imaging shows a heterogeneous mass that is hyperintense on T2 and demonstrates a honeycomb, heterogeneous enhancement with contrast. Treatment is surgical resection followed by radiation therapy. They are relatively radioresistant, and local recurrence is not uncommon.
Case contributed by Christopher Heald, UC M4
BACK TO
MAIN PAGE