Mycotic Aneurysm
Findings:
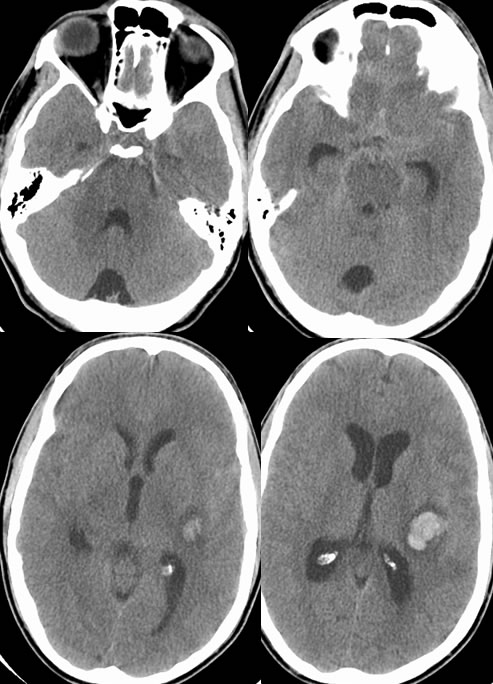
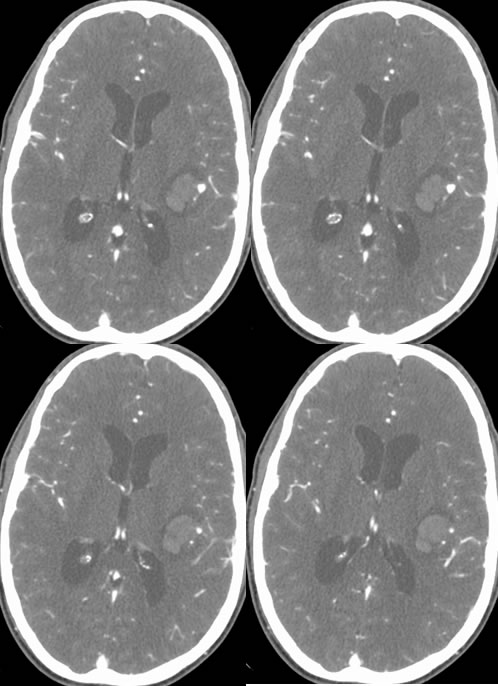
Noncontrast CT images demonstrate a moderate amount of suprasellar subarachnoid hemorrhage with evidence of mild hydrocephalus. A superimposed focus of parenchymal hemorrhage dissects into the posterior insula. Source images from the CTA demonstrate a globular focus of intense arterial enhancement along the lateral margin of the parenchymal hematoma. A follow up CTA five days later (not shown) demonstrated an increase in size of this aneurysm.
Differential diagnosis and discussion:
The differential diagnosis for intracranial hemorrhage is very broad. Underlying vascular causes include aneurysm, AVM/AVF, cavernoma, and hemorrhagic infarction either arterial or venous. The presence of a peripheral aneurysm without evidence of shunting should raise concern for a mycotic aneurysm which is typically caused by cardioembolism of aortic valve vegetation and/or bacteria in IV drug abusers. These aneurysms may also form in the setting of septicemia or contiguous infection, and are more common extracranially than intracranially. These are more appropriately termed pseudoaneurysms due to infection and partial disruption of the arterial wall and are prone to rupture, therefore if a peripheral aneurysm is elected not to treat initially, short term follow up CTA is indicated to exclude growth and need for more urgent intervention. Tumor emboli may rarely cause an oncotic aneurysm with similar natural history.