Fahr's Disease
nClinical:
nParkinson’s like movement disorder, headaches, dementia, vision, seizures, other neuropsychiatric symptoms beginning age 30-50 and progressive.
nPathology:
nRare (less than 20 families), autosomal dominant, no specific gene identified but likely related to abnormal phosphate transporter and/or PDGF and BBB, progressive with age
nConcentric calcium deposits in walls of small and medium size arterioles and might become occlusive
nExtensive gliosis without neuronal loss
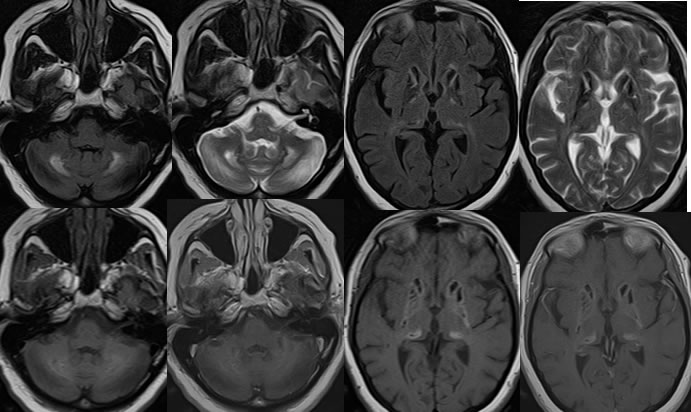
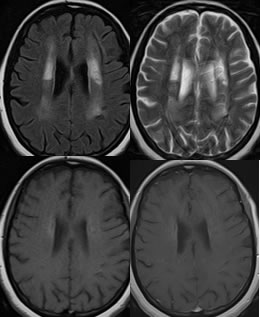
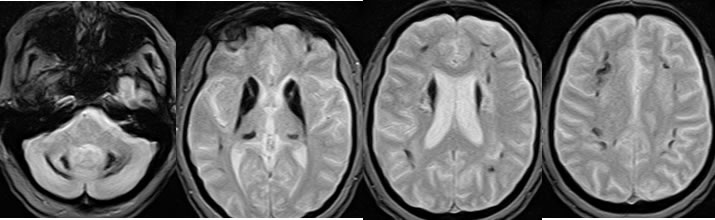
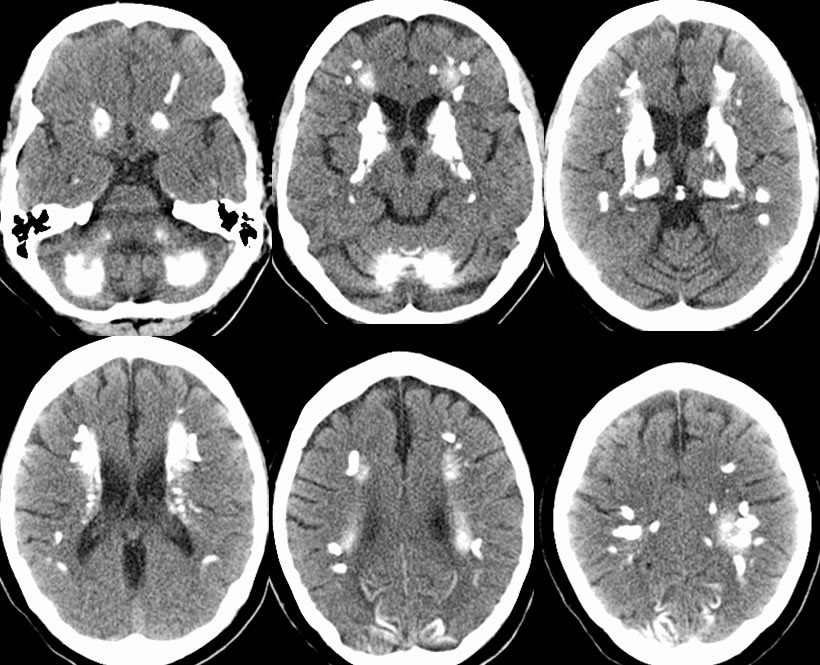
nImaging:
nCT- extensive symmetric calcifications basal ganglia, dentate nuclei, caudate, thalami, subcortical, cortex
nMR- complex signal of Ca++ in variable hydration state- hyper/iso/hypo
nMay be indistinguishable from hyperparathyroidism or other causes.
nDiagnostic criteria:
nBilateral basal ganglia calcification
nProgressive neurologic dysfunction
nNo other cause identified
nFamily history that suggest autosomal dominance
nRx/prognosis
nNo cure, symptomatic treatment, ?bisphosphonate, L-dopa ineffective, variable prognosis but typically long term disability
BACK TO
MAIN PAGE