Adenoid Cystic Carcinoma
Findings:
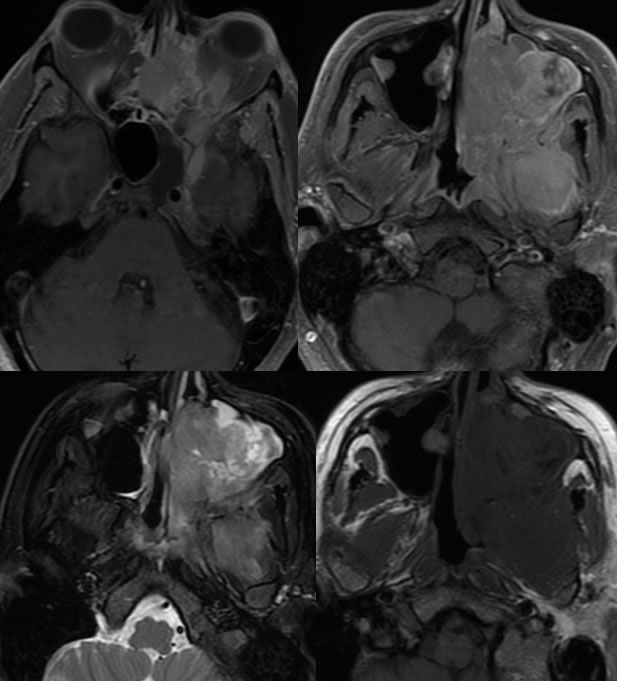
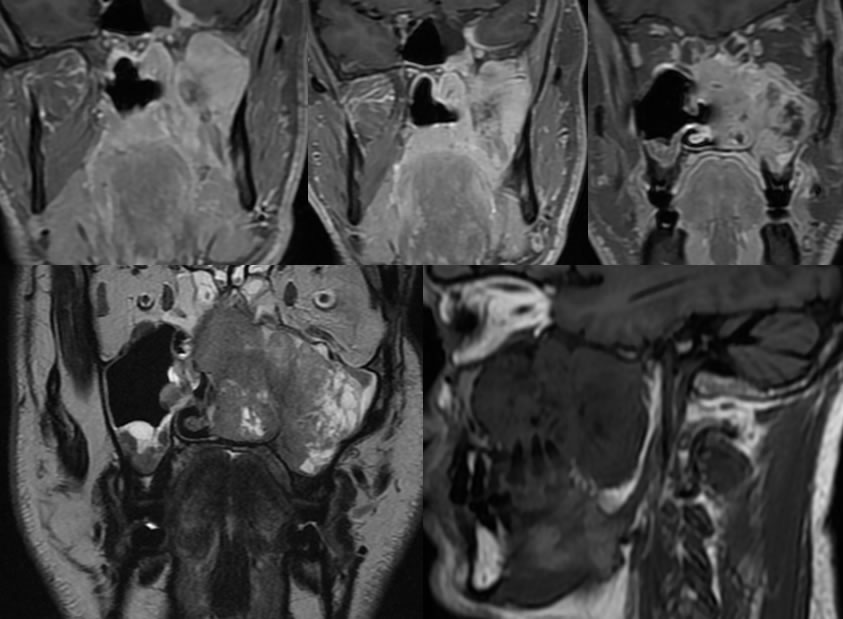
There is a large heterogeneously enhancing mass centered within the left maxillary sinus. This expands the left maxillary antrum and extends into the left nasal cavity as well as into the left greater than right ethmoid sinuses and left sphenoid sinus and sphenoethmoidalrecess. There is also involvement of the left medial and lateral pterygoidmusculature and extension into the anterior aspect of the left nasopharynx with asymmetric thickening and enhancement of the left superior aspect of the torus tubarius. There is demineralization of the anterior and posterolateral walls of left maxillary sinus, left lamina papyracea, and left orbital floor as well as erosion of the left maxillary tuberosity to involve the roots of the first through third left maxillary molar teeth, left posterior hard palate, and left medial and lateral pterygoidplates. There is abnormal enhancement and expansion of the left pterygopalatine fossa extending through the pterygomaxillary fissure and into the infratemporal fossa. Additionally, there is abnormal enhancement extending posteriorly within the foramen rotundum and vidian canal as well as within the inferior orbital fissure. There is extension of abnormal enhancement into the superior left buccal space with enhancement in the region of the left pterygomandibular raphe. There are multiple mucus retention cysts within the right maxillary sinus.
Discussion/Differential Diagnosis:
DDx: Salivary gland malignancy (adenoid cystic, mucoepidermoid, undifferentiated), sarcoma, lymphoma, less likely angiofibroma. The presence of perineuralspread indicates a malignant process.
Adenoid cystic carcinoma is most commonly seen in the parotid gland, but may be found in the submandibular gland or hard palate. They may also arise from minor salivary gland tissue. These lesions have nonspecific signal characteristics (T1 hypointense, T2 hyperintense), with homogenous enhancement that becomes more poorly defined with higher grade lesions and T2 signal that decreases with increasing cellularity and grade. A careful search for perineuralspread along cranial nerves 5 and 7/8 should be performed, since the presence of perineuraltumor worsens prognosis and decreases the likelihood of surgical cure. The presence of pain should raise suspicion for perineuralinvolvement, which may sometimes be noncontiguous with the primary mass. These tumors are typically slow growing but may have delayed recurrence and higher grade lesions may metastasize to lung and bone. Nodal metsare less common than systemic mets. Since they are slow growing, relatively prolonged survival may be seen even when metastatic, but 15 year survival rate is only about 38% overall. They are treated with wide surgical resection and radiotherapy.
This case was prepared with the assistance of Joshua Hall, UC undergraduate
BACK TO
MAIN PAGE