Esthesioneuroblastoma
Findings:
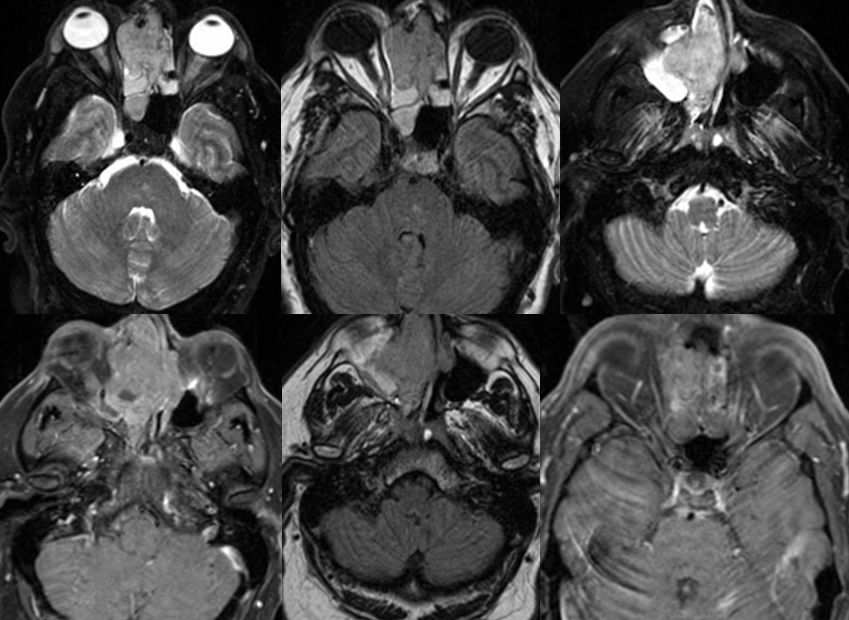
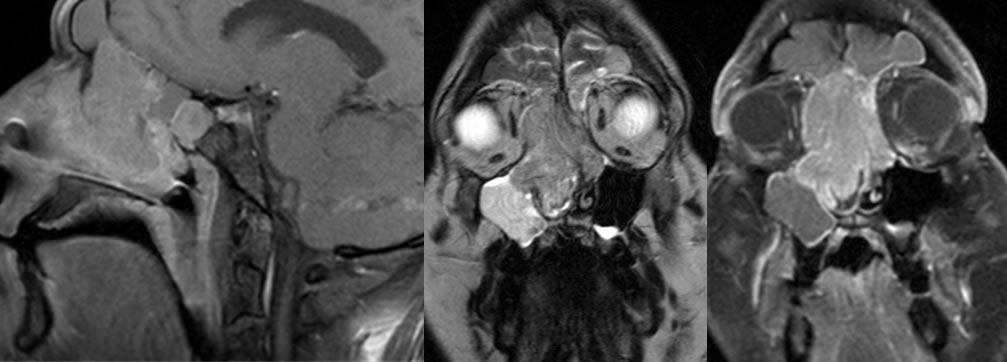
There is a large mildly hyperintense T2, hypointense T1 signal enhancing mass centered within the right nasal cavity, bilateral ethmoid, and right sphenoid sinuses which measures approximately 5.8 x 4.6 x 6.1 cm (craniocaudal by transverse by AP dimensions). This extends across the midline to the left nasal cavity and extends posteriorly on the right to the anterior right nasopharynx in the region of the torus tubarius. This results in expansion of the right nasal cavity and ethmoid sinuses with demineralization of portions of the medial right maxillary sinus wall, anterior right lamina papyracea, and right medial orbital wall with mass effect on the right medial orbit. There is thinning of the cribriform plate and portions of the anterior planum sphenoidale. There is minimal linear intracranial enhancement along the right inferior frontal lobe,likely dural involvement without definite brain parenchymal abnormality. The right pterygopalatine fissure is preserved. The mass extends to bilateral frontal recesses, without definite enhancing tissue within the frontal sinuses. There is extension to the right nasolacrimal duct. There is signal abnormality of the right maxillary sinus with a small area of enhancement along it's inferomedial wall. There is minimal layering fluid within the left maxillary sinus. There is no involvement of the hard palate. There is mild patchy opacity of the posterior ethmoid sinuses. No definite orbital apex involvement is noted. There is subtle associated radiologic proptosis of the right globe.
Discussion/Differential Diagnosis:
Differential Diagnosis: Esthesioneuroblastoma(ENB), Squamous Cell Carcinoma (enhance less than ENB, otherwise indistinguishable), Lymphoma (more homogenous, less enhancement than ENB, less skull base invasion), Nasal meningioma (look for hyperostosis),sinonasal undifferentiated neoplasm (indistinguishable by imaging)
Esthesioneuroblastoma (ENB) most commonly presents with epistaxis and nasal obstructive symptoms, with a bimodal distribution age 10-20 and 50-60, and a slight female predominance. The imaging appearance is somewhat nonspecific (aggressive mass with bone destruction, T1 hypointense, T2 hyperintense, necrosis), but the presence of cystic foci at brain/tumor interface of a dumbbell shaped lesion centered in the superior nasal cavity is classic. While intracranial extent is common, dural invasion is unusual. Stippled calcifications may occasionally be seen on noncontrast CT. ENB arises from neuroblasts within olfactory mucosa and are uncommon lesions, 2% of malignant nasal tumors with mets in up to 40% (nodes, bone, lung). Histologically, this is a small round blue cell tumor that simulates many other aggressive neoplasms (sarcoma, lymphoma, rhabdo, etc.), but the presence of neurosecretory granules on electron microscopy can be a helpful differentiating feature. Histologic grading is I-IV based on several morphologic features including degree of differentiation, mitotic rate, and presence of necrosis. They are staged by extent (Kadish- A-nasal cavity, B-nasal and sinuses, C- beyond nasal cavity +/- mets), and most are stage C due to delayed presentation. ENB is highly vascular and may bleed profusely when biopsied. They are treated with radical craniofacial resection and radiotherapy, with chemotherapy for higher grades and dissemination. Local recurrence is common (up to 60%), and survival rate correlates with grade and stage as would be expected. Stage C lesions lead to a less than 50% 3 year survival.
This case was prepared with the assistance of Joshua Hall, UC undergraduate
BACK TO
MAIN PAGE