Primary Thyroid Lymphoma
Findings:
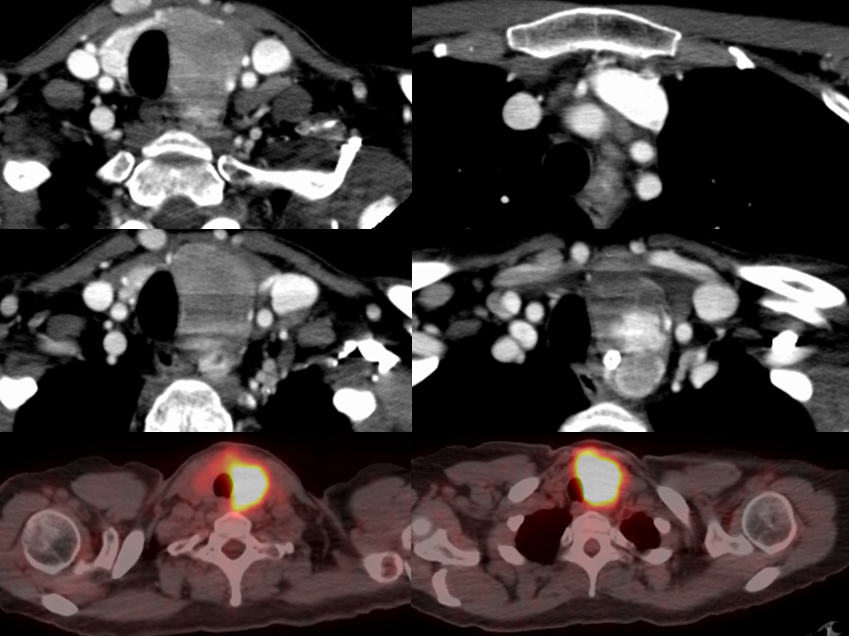
Axial contrast enhanced neck CT images demonstrate a large infiltrative nearly homogeneous mass within the left thyroid lobe which is superimposed upon heterogeneous nodularity of the left thyroid lobe extending into the thoracic inlet. The infiltrative mass shows marked FDG uptake on PET compared to the right thyroid tissue.
Differential Diagnosis:
Thyroid lymphoma, medullary thyroid carcinoma, anaplastic thyroid carcinoma (more heterogenous, necrotic, calcification). The more common differentiated thyroid cancers (papillary, follicular) are typically more heterogenous and may be complex cystic/solid, but there is some overlap of appearance and a more homogenous lesion may be seen occasionally if small.
Discussion:
Primary thyroid lymphomas almost entirely present as B cell non-Hodgkin lymphoma in the setting of an autoimmune disorder, usually Hashimoto’s Thyroiditis. Clinical presentation is typically in women with a median age of 60 with a rapidly enlarging thyroid mass. A single mass is much more common than multiple lesions. A diffusely infiltrative lymphoma may be indistiguishable from Hashimoto’s Thyroiditis on a single study, but rapid enlargement should raise the possibility of lymphoma.
Contrast CT Imaging will likely show a hypodense homogenous or slightly heterogenous mass which enhances less than normal thyroid. Necrosis and calcification are uncommon. The lesions may invade the carotid sheath and/or metastasize to adjacent lymph nodes, but more commonly compress rather than invade adjacent structures. Ultrasound will show a uniformly markedly hypoechoic lesion that may simulate a cyst if there is not careful attention to technique. PET CT or Gallium scan will show increased uptake compared to normal tissue, while this lesion will be cold on other NM studies (Tc99m, I-123). Lymphoma is the only thyroid malignancy that demonstrates intense Gallium uptake. MRI will often be hyperintense to normal surrounding the thyroid gland on T2 weighted images while T1 will often appear isointense, with diffuse low level enhancement after gadolinium.
Fine needle aspiration may be used for diagnosis, buy may be difficult to distinguish from Hashimoto’s, requiring surgical biopsy for definitive diagnosis. Staging is considered IE (extranodal solitary) if limited to thyroid and IIE when spread beyond thyroid. Thyroid Lymphoma is typically treated without surgery unless needed for palliation of large lesions causing obstructive symptoms. 3 – 6 courses of R-CHOP regimen chemotherapy followed by radiation therapy are effective in up to 90%, but response is poorer for stage IIE with 35% FYSR. Patient age also correlates with survival.
This case was prepared with the assistance of Joshua Hall, UC undergraduate