Extensive Prominent Perivascular Spaces
Findings:
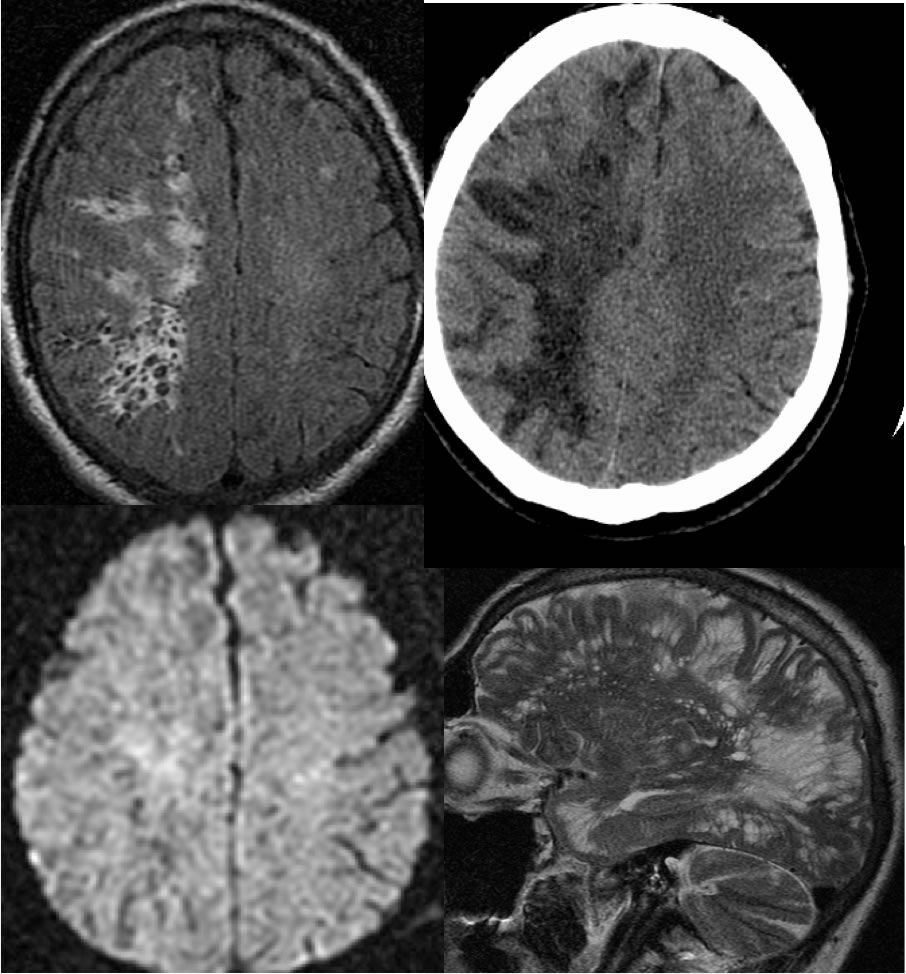
Extensive radiating tubular foci of CSF signal intensity extend throughout the right cerebral hemispheric white matter, associated with surrounding FLAIR hyperintensity. There is no associated mass effect or significant overlying cortical volume loss. This process shows diffuse low attenuation on CT. Fine linear septations are seen within this process on the sagittal T2 weighted imaging.
Differential Diagnosis:
Ovoid/linear zones of CSF signal cavitation within the white matter may be seen with prominent perivascular spaces and remote insults including remote lacunar infarctions. The characteristic location and morphology of perivascular spaces helps to make the distinction.
Discussion:
Type I perivascular spaces (PVS) are very commonly seen within the inferior basal ganglia and may be symmetric. Type II PVS follow the course of medullary arteries in the convexities and radiate from the ventricular system into the subcortical region. Type III PVS are seen within the midbrain and other brainstem structures. These findings may have a bizarre appearance that simulate neoplasm or other cystic mass, and may also asymmetrically involve one hemisphere as in this case. Hydrocephalus may result if the cerebral aqueduct is compressed by massive type III PVS. Perivascular spaces are differentiated from other causes by the signal characteristics and characteristic location. Reactive gliosis along the margins of perivascular spaces is common and may be extensive, simulating surrounding vasogenic edema or demyelination in some cases. If prominent type I PVS are seen in immunocompromised patients, cryptococcal infection could be considered.
(Kwee et al. Radiographics July 2007 27(4):1071-1086).
BACK TO
MAIN PAGE