Rosette Forming Glioneuronal Tumor
Findings:
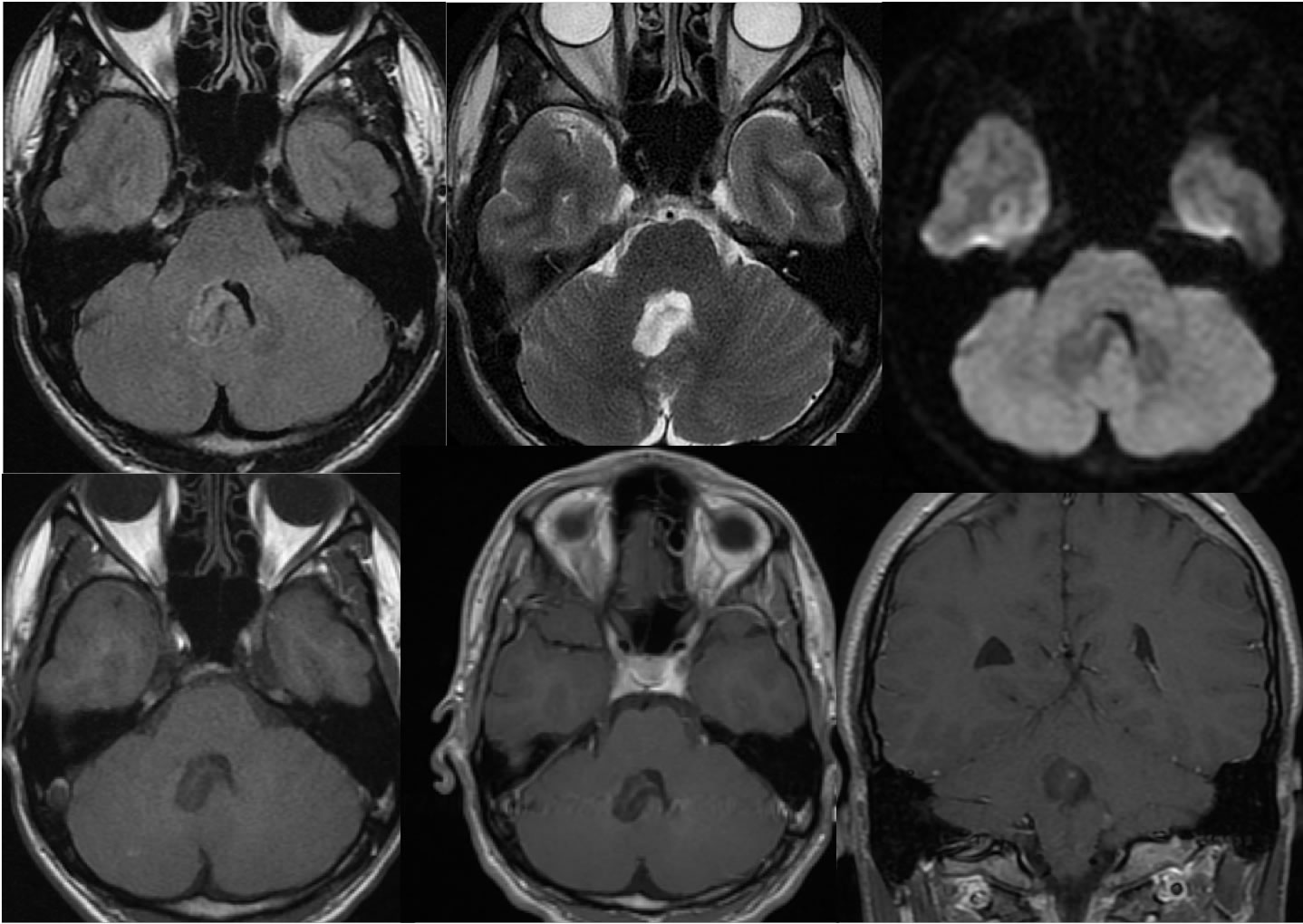
Multiple MRI images demonstrate a heterogeneous mass within the right aspect of the fourth ventricle causing mild expansion of the fourth ventricle. A tiny eccentric zone of enhancement is seen on coronal imaging. No diffusion restriction is seen.
Discussion/Differential Diagnosis:
The differential diagnosis for a nonenhancing or minimally enhancing fourth ventricular mass is relatively broad and is tailored by the age of the patient. The primary differential diagnosis for this lesion is a pilocytic astrocytoma, but is not the classic appearance of a cystic lesion with enhancing mural nodule. A ganglioma or gangliocytoma could appear similar, but are more common in the supratentorial compartment. Pleomorphic xanthroasrocytomas are nearly always supratentorial.
Rosette forming glioneuronal tumors are rare, indolent, and most common within the fourth ventricle and aqueduct region in young adults. They present with symptoms of obstructive hydrocephalus, or may be asymptomatic and discovered incidentally. These lesions have variable solid and cystic components, but are most commonly solid or mixed solid and cystic. 25% may show some calcification on CT. Variable enhancement of the solid components is seen on MR. These tumors appear well circumscribed but are locally invasive, and are curable with complete resection. The histology reflects glial and neurocytic components as the name suggests, with a low Ki-67 proliferation index. These are considered WHO grade 1 lesions.
BACK TO
MAIN PAGE