Head and Neck Cancer, Nodal Metastases
Findings:
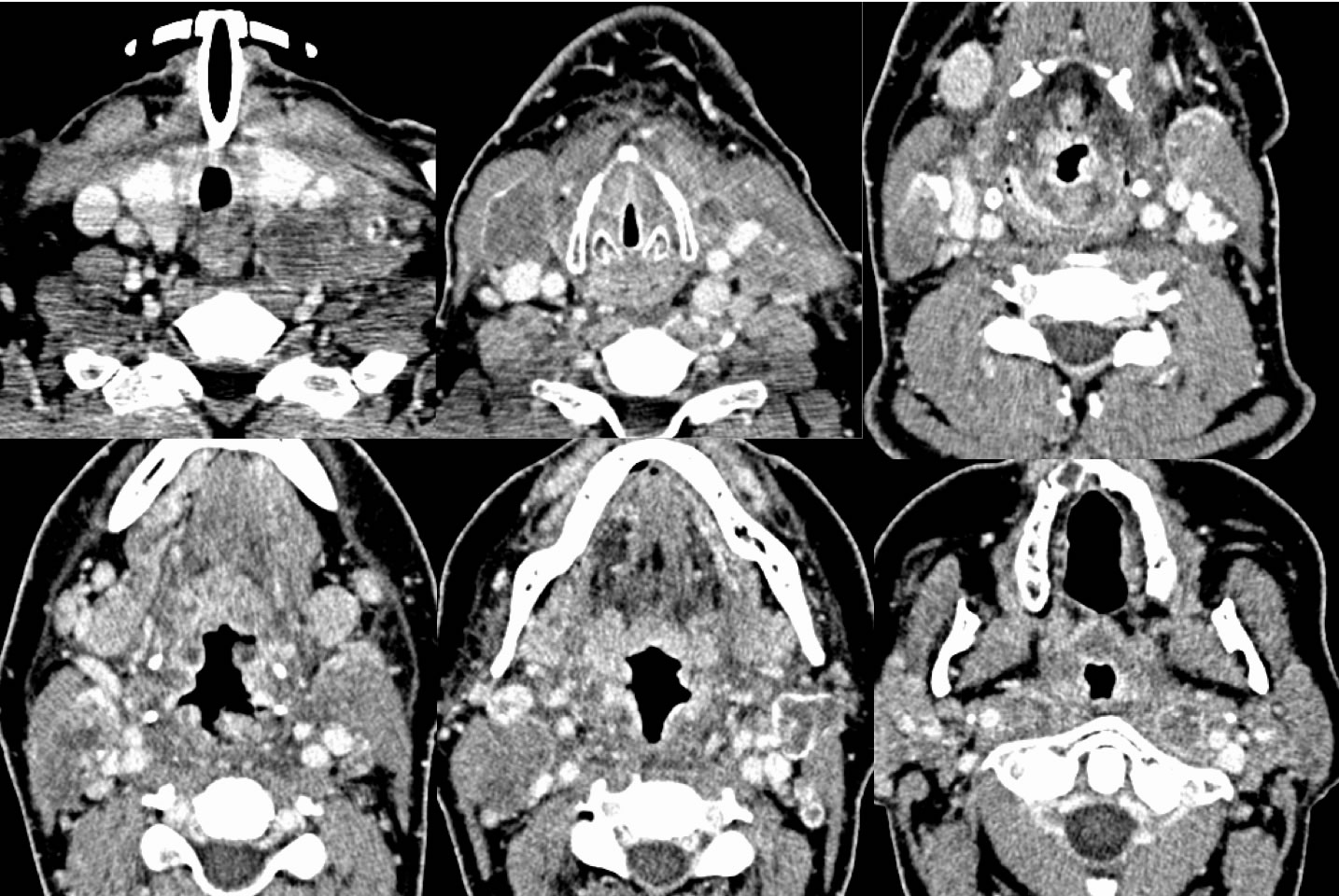
Axial contrast enhanced neck CT images incompletely demonstrate a tracheostomy in place, with extensive bilateral solid and centrally necrotic abnormal lymph nodes involving retropharyngeal regions, bilateral level 2, and left level 3-5. There is diffuse irregular enhancement and thickening of the oropharyngeal mucosal surfaces with some zones of ulceration suspected. Some of the lymph nodes demonstrate irregular margins and are inseparable from adjacent structures, suspicious for extracapsular nodal spread.
Discussion:
The prognosis and treament of head and neck cancer is affected by primary tumor local extent, presence/extent of nodal metastases, and presence of extranodal metastatic disease, as well as comorbidities. Nearly 50% of patients with oral cavity squamous cell carcinoma have nodal disease. Extracapsular nodal spread (ECS) is known to worsen prognosis and may be diagnosed on imaging when the tumor extends clearly beyond the nodal capsule and invades adjacent tissues. ECS may be macroscopic or microscopic, and has been given a threshhold of approximately 1.7 mm to reach clinical relevance. Survival in patients with ECS is improved with postop chemoradiation over PORT despite higher toxicity. Reference:Wreesmannn et al. Head Neck 2016 Apr;38(Suppl 1):E1192-E1199.
BACK TO
MAIN PAGE