Perineural Tumor Spread, Melanoma
Findings:
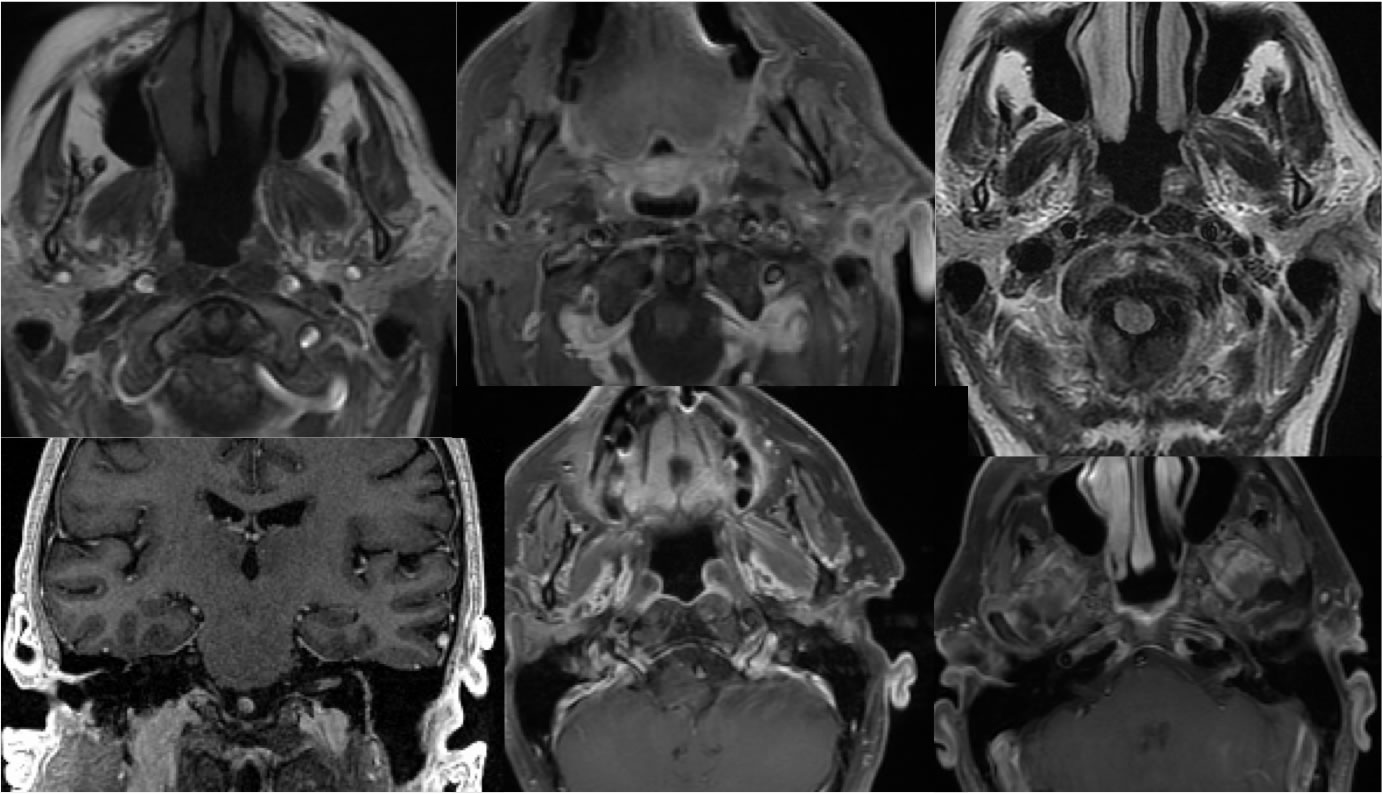
MR images without and with fat saturation demonstrate postoperative changes of partial left parotid resection. Abnormal enhancement is present within the parotid bed. There is diffuse slightly irregular abnormal enhancement of the left facial nerve extending into the internal auditory canal.
Discussion/Differential Diagnosis:
Perineural spread of malignancy (PNS) is associated with worsened prognosis and increased risk of locoregional recurrence. Perineural invasion (PNI) is another term that is sometimes used interchangeably but should be reserved for pathologic diagnosis of microscopic tumor spread along small nerves that are not visible on imaging. While adenoid cystic carcinoma is the "classic" tumor associated with PNI, occuring in up to over 90% of cases, squamous cell carcinoma(SCC) is by far the most common overall cause of PNI being the most common malignancy in the head and neck. PNI may be seen in up to 80% of SCC. Non squamous skin or salivary gland cancers such as melanoma may also cause PNS. Known neural supply of the region of primary tumor should be closely inspected for the presence of asymmetric enhancement, loss of T1 hyperintense fat plane, and nodularity. This includes the auriculotemporal and facial nerves for parotid lesions, foramen ovale for nasopharyngeal/oropharyngeal lesions, and foramen rotundum as well as infraorbital nerve for anterior facial lesions. Discontiguous involvement is common, including Meckel's cave and cavernous sinus.
BACK TO
MAIN PAGE