Gliomatosis Cerebri
Findings:
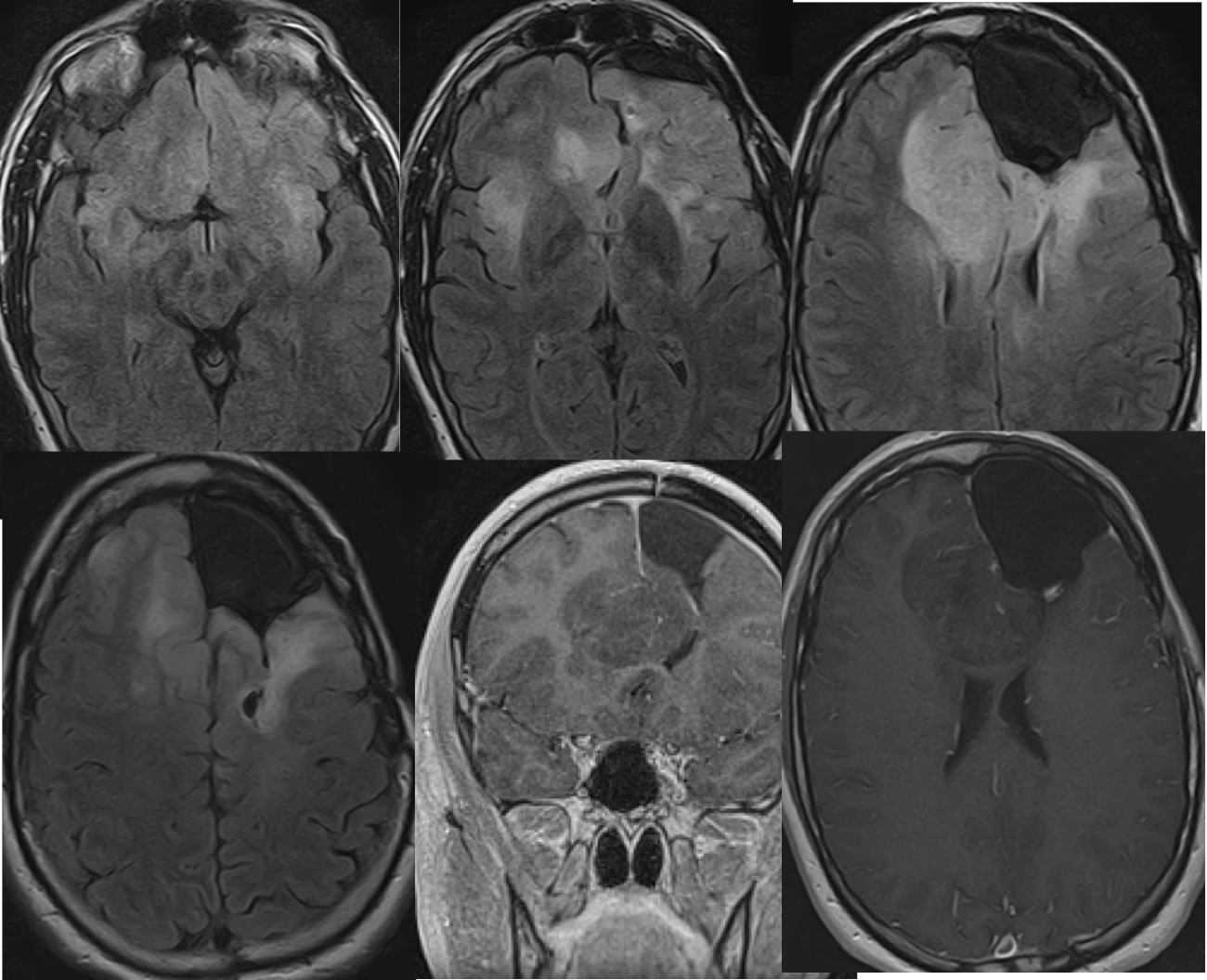
Four axial FLAIR, coronal T1 postcontrast and axial T1 post contrast images demonstrate postoperative findings of left frontal craniotomy. Nodular nonenhancing signal abnormalities extend along the margins of the surgical defect, involving the anterior corpus callosum with marked expansion. Additional hazy nodular signal abnormalities involve the right frontal lobe and bilateral insula. A few spotty zones of enhancement are present along the margins of the surgical defect.
Discussion/Differential Diagnosis:
Despite being recognized since 1938, Gliomatosis cerebri (GC) remains controversial regarding definition, histology, and treatment. It is typically thought of as a diffuse infiltrating glioma that involves multiple (3 or more) lobes of the brain with clinical symptoms less than expected for the extent of involvement. There is agreement that the prognosis is poor regardless of treatment. It is no longer recognized as a distinct entity in the 2016 WHO classification, but is now considered a growth pattern of diffuse glioma. The 2016 WHO subclassifies GC growth patterns according to histologic grade and molecular findings. GC may arise primarily or as a manifestation of tumor recurrence/progression after radiation and/or antiangiogenic therapy. Many other examples of glial malignancy are found on this site.
Condensed from Ranjan, S and Warren, K; Gliomatosis Cerebri: Current Understanding and Controversies. Oncol. 2017;7:165
BACK TO
MAIN PAGE