Angiofibroma
Findings:
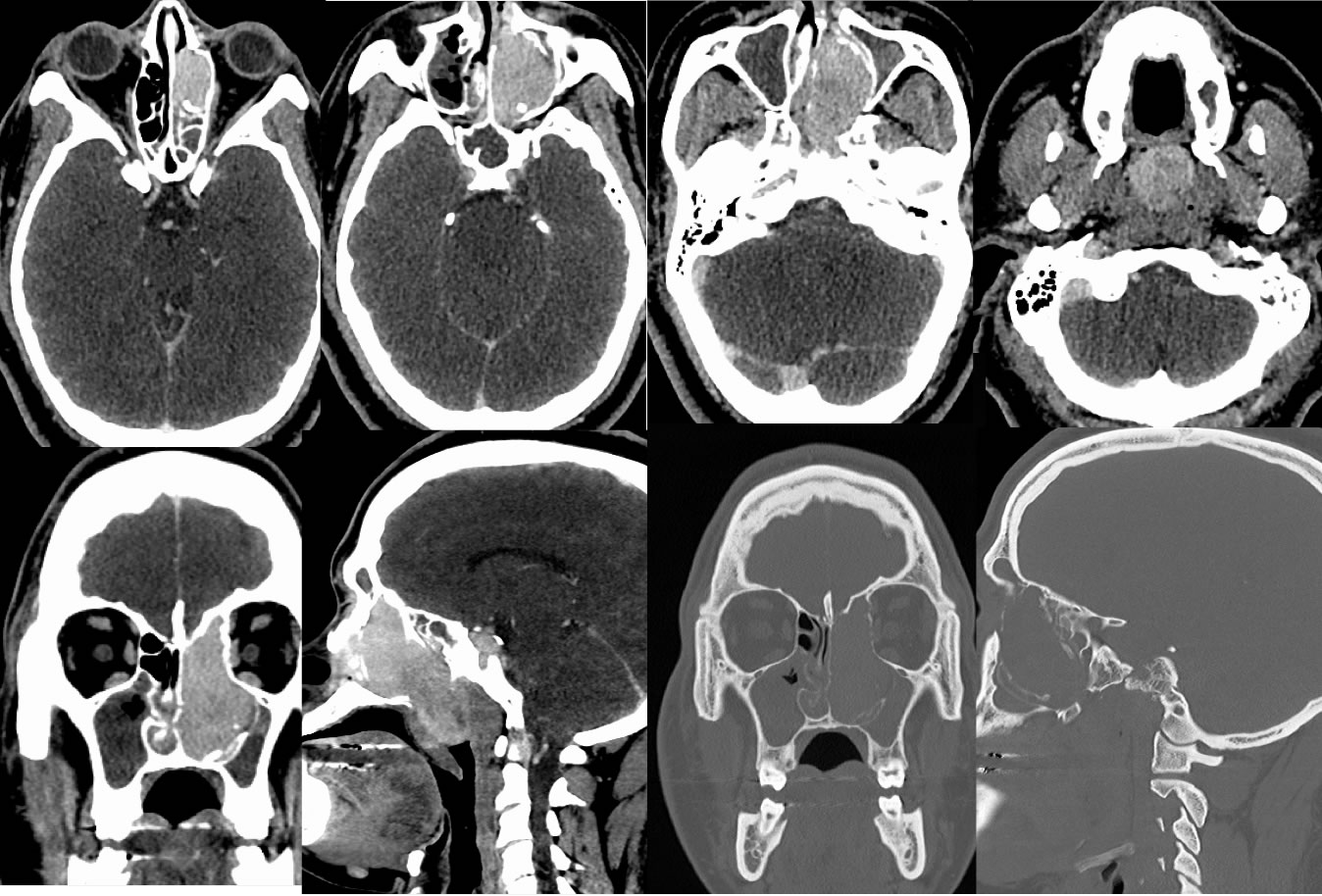
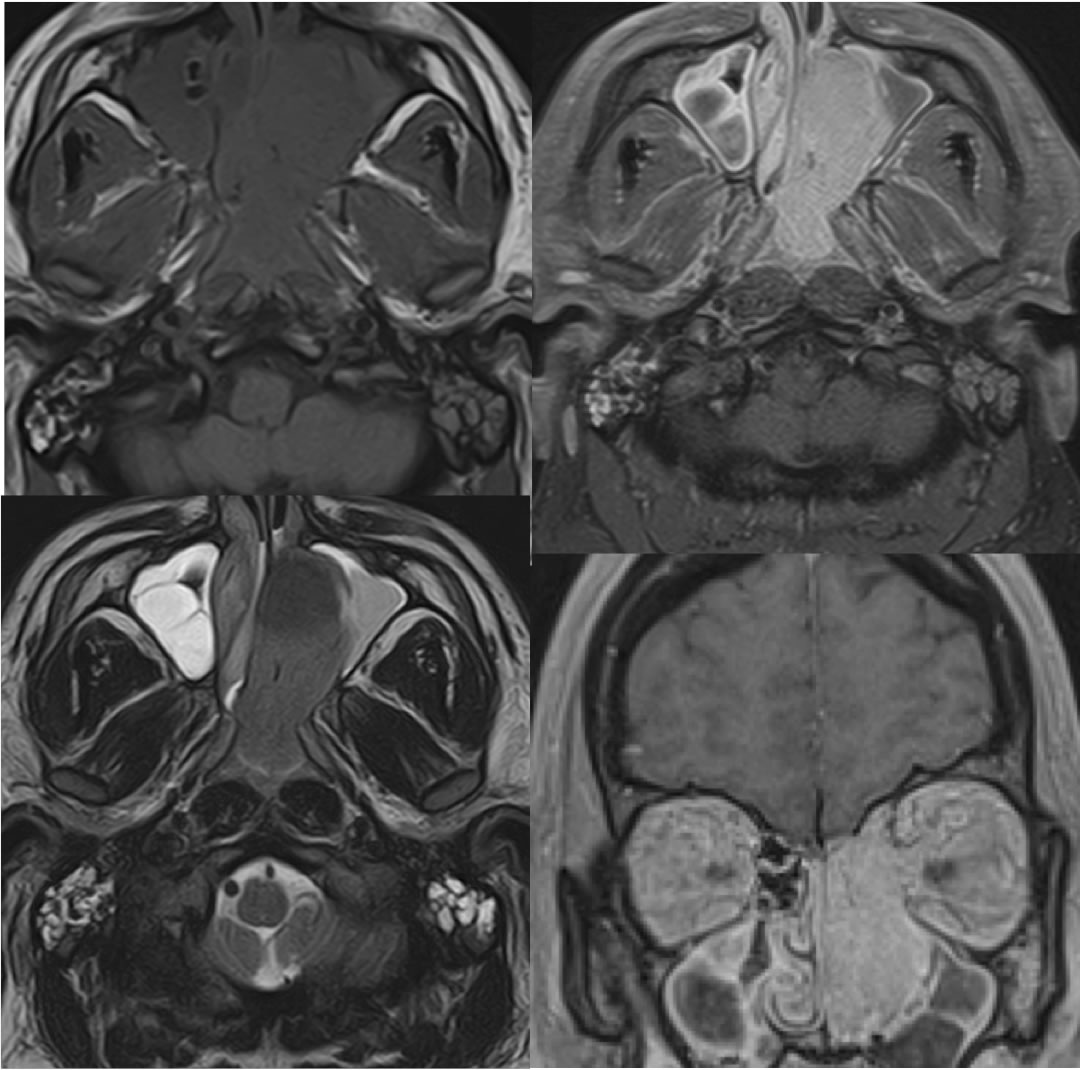
Contrast enhanced CT images of the neck, including coronal and sagittal reformats with bone algorithm demonstrate a large intensely enhancing mass within the left nasal cavity and ethmoid air cells extending into and occluding the nasopharynx. Postobstructive low density inflammatory disease is present in the left maxillary and sphenoid sinuses and there is low-density inflammatory disease within the right maxillary sinus. The mass is expansile and causes bone remodeling and some zones of bone destruction. Definite intracranial extent is not seen. The corresponding MR images demonstrate overall low T2 signal of the mass, with intense enhancement after gadolinium. The mass demonstrates different signal than the zones of inflammatory disease in the paranasal sinuses and mastoid air cells.
Discussion/Differential Diagnosis:
The differential diagnosis for this mass includes angiofibroma, rhabdomyosarcoma, nasopharyngeal carcinoma, esthesioneuroblastoma. The latter three would be expected to have a more aggressive bone destruction pattern with no remodeling and perhaps less intense hypervascular enhancement. Polyps, encephalocele, lymphangioma would not enhance. Teratoma would be more heterogenous.
Angiofibromas, also known as Juvenile Nasopharyngeal Angiofibromas are rare, benign but locally aggressive, hypervascular tumors seen almost exclusively in adolescent males. While rare overall, they are the most common benign tumor of the nasopharynx. Clinically these may present with severe epistaxis and/or obstructive symptoms. Biopsy may cause catastrophic hemorrhage. These typically arise near the sphenopalatine foramen with anterior bowing and remodeling of the posterior maxillary wall. Local extent may be significant, including intracranial invasion. These tumors are surgically resected with preop embolization, with a high recurrence rate if it involves the skull base. Radiotherapy may be helpful for control of residual and recurrent tumor. Atypical features of this particular lesion include homogeneity with few visible flow voids and origin from the nasoethmoid region rather than the sphenopalatine foramen. In addition, this is not obvious but this patient is an early middle age adult, therefore outside the typically expected age group.
BACK TO
MAIN PAGE