Fungal Encephalitis, Zygomycetes spp.
Findings:
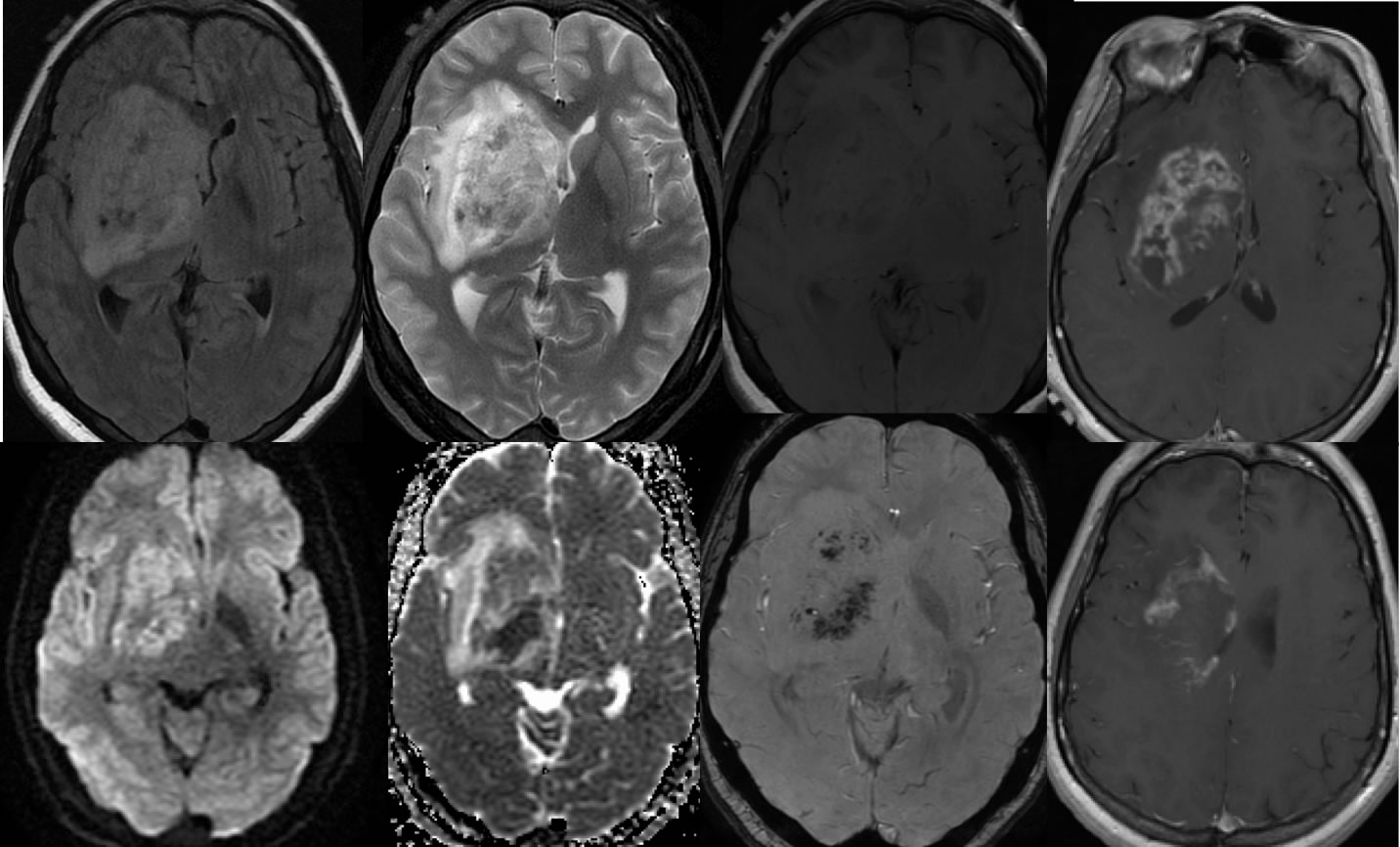
Multiple MR images demonstrate a poorly defined masslike lesion within the right basal ganglia and caudate region with mass effect and surrounding edema. Mixed diffusion signal is seen with some areas of T2 shine through and other areas of true restricted diffusion. Spotty hypointensities are seen within this lesion on the gradient echo sequence. The process demonstrates patchy very poorly defined enhancement without a well-defined nodular mass. Subependymal enhancement is also seen. Complex signal is seen on T2 weighted imaging, with areas of increased and decreased signal. Some of the zones of decreased T2 signal correlate with hypointensities on the gradient echo image.
Discussion/Differential Diagnosis:
The differential diagnosis for this process is broad including infection, metastatic or primary neoplasm, and a subacute infarct. The presence of the mixed diffusion signal, patchy poorly defined and not nodular enhancement, and spotty T2* hypointensties would be unusual for neoplasm and more typical for an infectious process. The mass effect is greater than would be expected for a subacute infarct, and the signal changes are not really compatible with a subacute infarct. Of the infectious processes, fungal disease most commonly has the spotty T2* hypointensities correlating with hemorrhagic changes and metal ions.
Cryptococcus is the most common CNS fungal infection, typically seen in immunocompromised and most commonly presenting as a meningitis. Fungal cerebritis may be caused by cryptococcus, aspergillus, candida, and other species including zygomycetes. The few cases of zygomycetes encephalitis available in search and my collection appear to have similar imaging features, including a predilection for the lentiform nuclei often bilateral, patchy poorly defined enhancement, mixed attenuation on CT, and T2* spotty hypointensties correlating with hemorrhagic changes and metal ions.
BACK TO
MAIN PAGE