Diving Ranula
Findings:
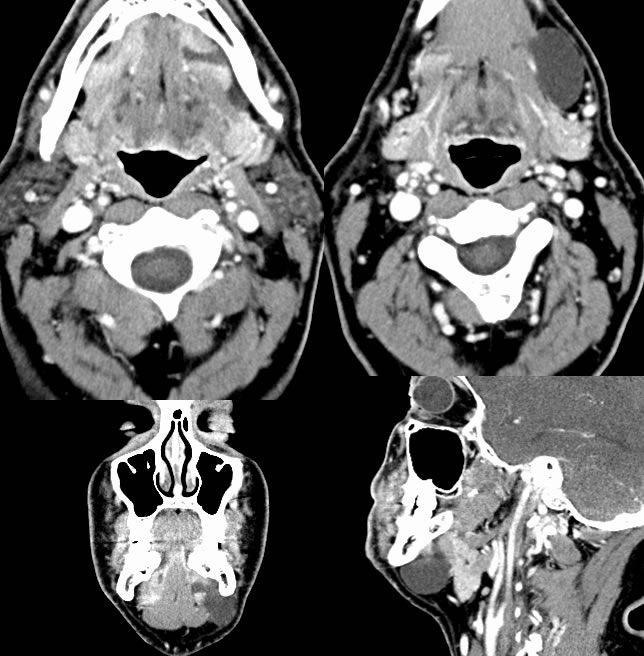
Multiple axial and coronal neck CT images demonstrate a well-defined focus of water attenuation within the left submandibular region which has an imperceptible wall and has a thin connection to the left sublingual gland. The structure extends below the mylohyoid muscle and is medial to the platysma.
Discussion/Differential Diagnosis:
The lack of enhancement excludes a large number of lesions that can present in the submandibular region. Simple fluid attenuation with an imperceptible wall indicates a simple cystic structure, and from that point the etiology can be determined by the locaton and morphology of the lesion. This lesion has a clear connection to the sublingual gland indicating an origin from the sublingual gland as a sialocele variant, a ranula. The mylohyoid muscle demarcates whether this is a simple or diving ranula. Diving, cervical, or plunging ranula extends below the level of the mylohyoid muscle. These are pseudocysts (lined by connective tissue and not epithelium) resulting from obstruction of a sublingual or minor salivary gland duct in the floor of mouth. This may be caused by trauma, surgery, or be idiopathic. When these become superinfected and/or contain hemorrhagic products, they may have more complex attenuation and signal and may simulate neoplasm. When superinfected, these have the appearance and clinical symptomatology of abscess. The connection of the lesion to the floor of mouth is an important feature to distinguish from other etiologies, and may be subtle due to decompression into the submandibular space. These are treated surgically, with a high recurrence rate unless both the cervical and oral components are addressed. Complete intraoral removal of the gland and drainage of the cyst is reliably curative.
BACK TO
MAIN PAGE