Metastatic lung cancer with L vocal cord paralysis
Findings:
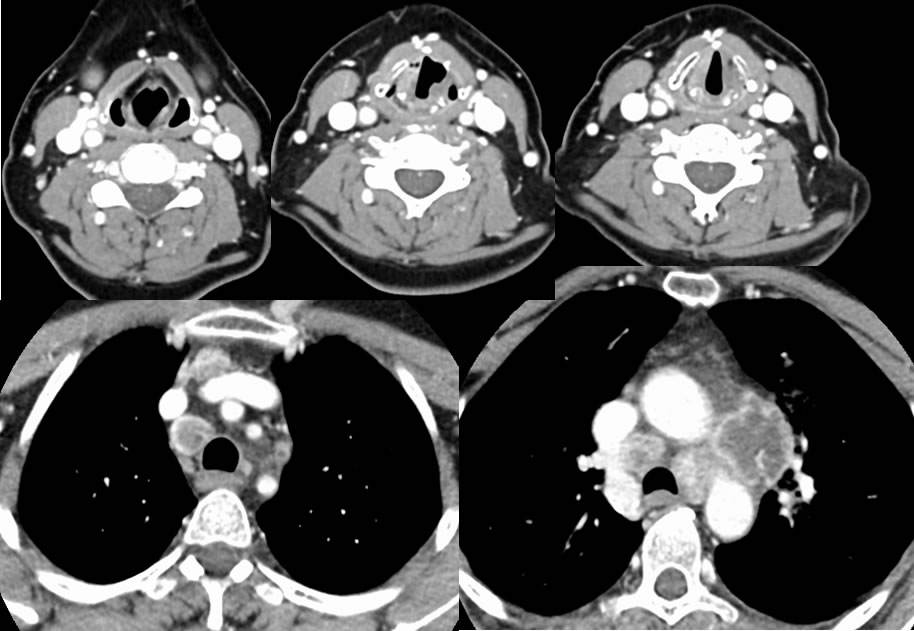
An irregular centrally necrotic mess infiltrates the AP window. Centrally necrotic adenopathy is also present within the mediastinum. There is slight dilation of the left pyriform sinus with abnormal medial position of the left aryepiglottic fold. The left vocal cord is in an abnormal paramedian position and there is a "sail sign" within the laryngeal ventricle, findings compatible with vocal cord paralysis related to the mass involving the expected course of the left recurrent laryngeal nerve.
Differential Diagnosis:
Lung cancer, mediastinal abscesses, metastases from unknown primary.
Discussion:
True vocal cord (TVC) paralysis or paresis is associated with some combination of abnormal paramedian position of the affected vocal cord, triangular aeration of the laryngeal ventricle sometimes described as a “sail sign”, anterior position of the arytenoid cartilage, thickening and medialization of the aryepiglottic fold, asymmetric dilation of the ipsilateral pyriform sinus, and volume loss in the immediate subglottic region. Despite these characteristic imaging findings, the presence of TVC paralysis is readily appreciated on clinical inspection. Therefore the role of the radiologist is typically not to diagnosis TVC paralysis, but to search for an underlying cause which may be anywhere along the course of the recurrent laryngeal nerve (RLN). The RLN arises from the vagus nerve and loops under the aortic arch on the left and under the subclavian artery on the right to ascend in the posterior tracheoesophageal groove to provide most of the motor supply to the larynx. In the case of an aberrant right subclavian artery, there will be no right RLN since the anomalous right laryngeal nerve then branches from the vagus at the level of the larynx. Imaging workup should include contrast neck CT at least through the level of the AP window. TVC paralysis is most commonly unilateral and on the left, with 1/3 caused by tumors, 1/3 traumatic, and 1/3 idiopathic. An isolated superior laryngeal nerve palsy if suspected by the ENT specialist should direct the search more superiorly to the intracranial compartment, as should the presence of other palsies. Bilateral TVC paralysis is rare and life threatening, caused by iatrogenic surgical complications including intubation, trauma, and neurodegenerative/neuromuscular diseases.