Multiple Cavernomas
Findings:
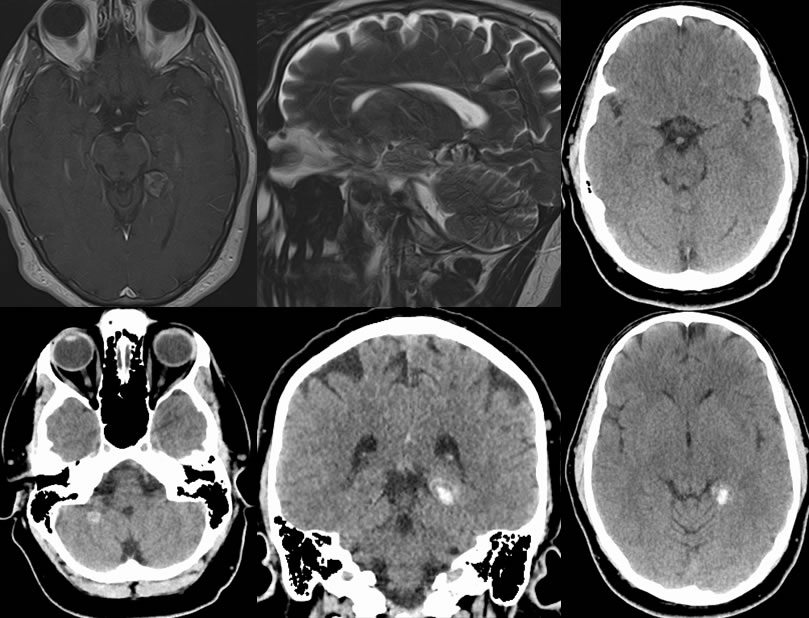
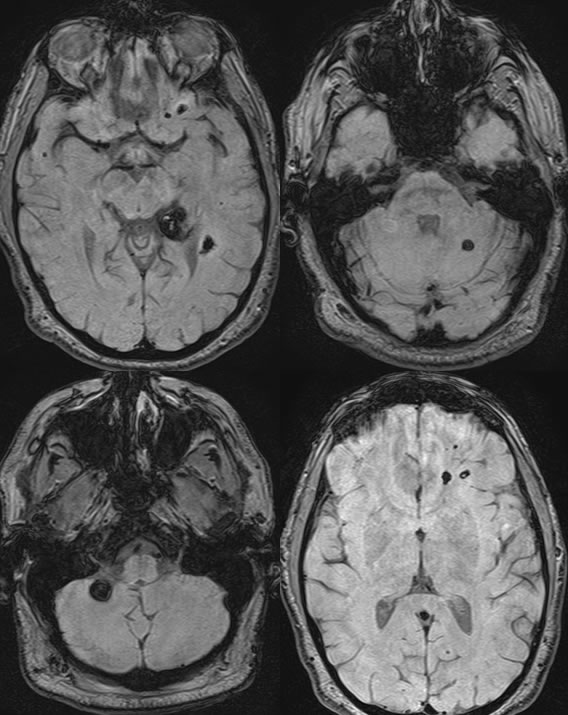
CT images show a hyperdense lesion within the left posterior medial temporal lobe, which measures approximately 1.7 x 1.7 cm. This abuts the left tentorial leaflet but does not definitely appear extra-axial. There are tiny foci of slightly higher density centrally. There is a tiny hyperdense lesion within the right cerebellar hemisphere inferiorly, which measures approximately 0.7 cm. This does not have any characteristics of an extra-axial lesion. There are 2 tiny foci of hyperdensity within the left frontal lobe which measure approximately 1-2 mm.The MR images demonstrate multiple additional smaller lesions which are less well seen on CT, in particular the black blood sequence which demonstrates multiple lesions. The dominant lesion on the left has a thick hemosiderin rim and internal stippled T2 hyperintensity, with minimal internal enhancement.
Discussion/Differential Diagnosis:
This patient presented with a history of trauma, which can be problematic given the hyperdensities on CT that simulate more acute hemorrhage. Cavernomas, more appropriately termed cavernous malformations (CM), are rare in the spinal cord and most common intracranially, presenting with seizures in 50% although 20% may be asymptomatic. Other neurologic deficits may be seen which might correlate with more acute hemorrhage. Natural history is heterogeneous, with hemorrhage and de novo lesions occurring more frequently if hereditary. 75% are solitary, 10-30% multiple/familial, with autosomal dominant mutations localized to chromosomes 3 and 7q. The characteristic imaging appearance is that of a thick surrounding hemosiderin rim with a stippled popcorn like T2 MR core, little or no detectable enhancement, hyperdense on CT and possibly partially calcified (60%), occult on CTA/DSA. GRE is most sensitive for detection of very small lesions which may appear similar to microhemorrhage of other cause. Acute hemorrhage related to CM has a nonspecific appearance simulating many other causes. Histologically, CM are epithelial lined blood filled sinusoidal spaces within a collagenous matrix, showing hemorrhage of various stages. Grading system is as follows (Zabramski):Grade 1- subacute hemorrhage, Grade 2- mixed age hemorrhage, Grade 3- chronic hemorrhage, Grade 4- punctate foci seen on GRE. Unlike cavernous hemangiomas, CM are nonproliferative lesions. The lesions are treated with microsurgical resection with XRT having a limited role. Care must be taken to avoid disrupting commonly associated developmental venous anomalies (DVA), which may cause venous infarcts due to the DVA draining normal brain. Additional examples of CM are found here and here.
This case was prepared with the assistance of Joshua Hall, UC undergraduate.
BACK TO
MAIN PAGE