Ameloblastoma
Findings:
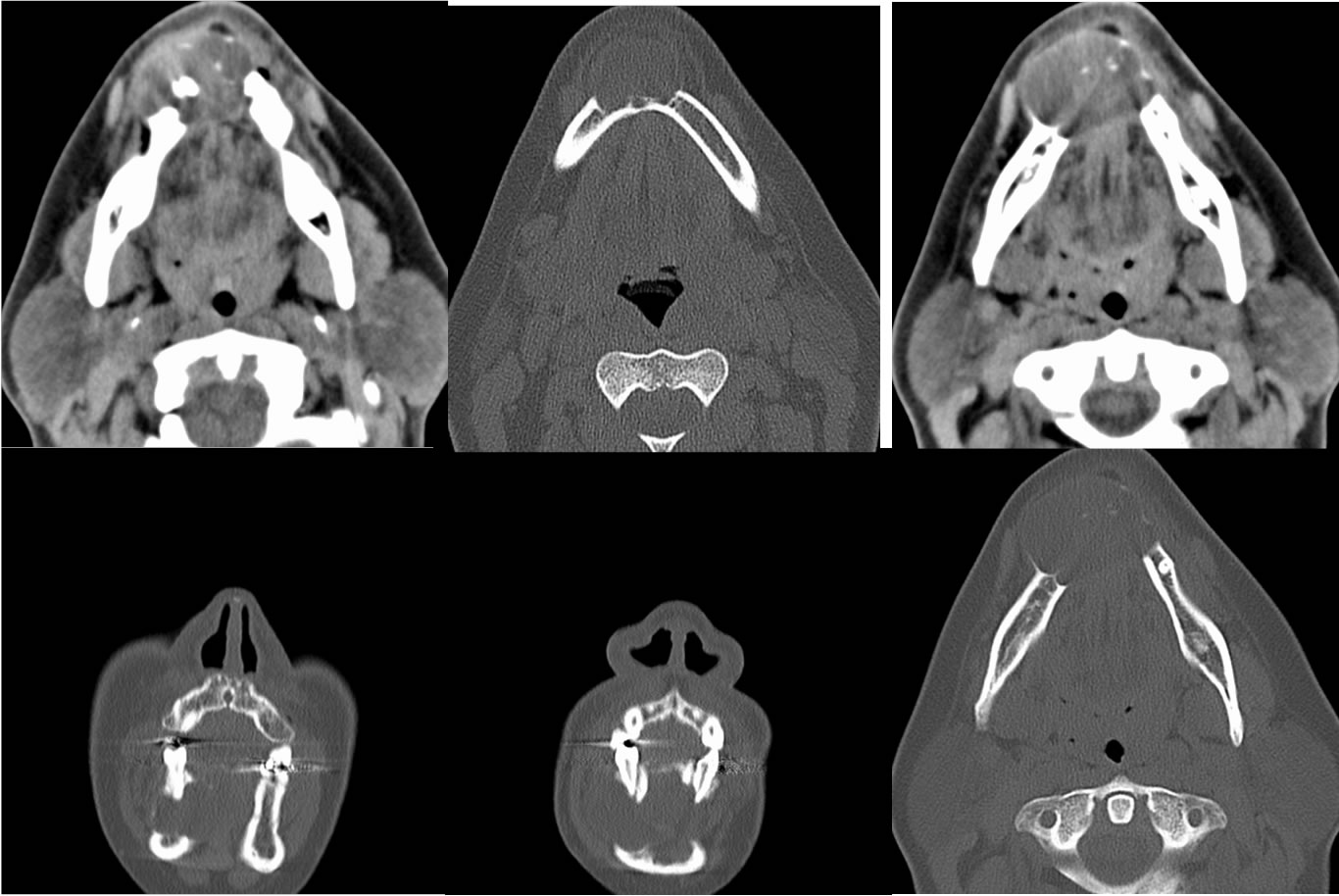
Multiple axial and coronal CT images demonstrate an expansile lytic lesion involving the midline anterior mandible with a few internal calcifications. There is some bone remodeling, but the lesion is markedly expansile with several areas of bone interruption and other areas with imperceptibly thin cortex.
Discussion/Differential Diagnosis:
Expansile lytic lesion with cortical interruptions, unilocular or multilocular, with or without soft tissue mass
Slowly growing and painless, mandible>>maxilla, 30-50 yo most commonly.
Second most common odontogenic tumor behind odontoma but still rare.
Path- benign histology but locally invasive, histologically very similar to craniopharyngioma.
Imaging-CT expansile lytic multisepatated, MR nodular peripheral enhancing to dist from other lesions.
En-bloc resection due to local curettage having high recurrence rate (45-90%).
Malignant, more aggressive variants: ameloblastifc carcinoma, malignant ameloblastoma (mets)
Ddx of mandibular cystic lesions:
Dentigerous cyst- crown of unerupted tooth (some amelo may arise from preeexisting dentigerous cyst)
Radicular cyst- roots- most common- caries
Odontogenic keratocyst- more aggressive, multilocular, impacted tooth, thin poorly enhancing walls
Odontogenic myxoma- may be indistinguishable
Others: ABC, giant cell granuloma, fibrous dysplasia
Additional cases:
-ameloblastoma
-ameloblastoma2
BACK TO
MAIN PAGE