Neuromyelitis Optica
Findings:
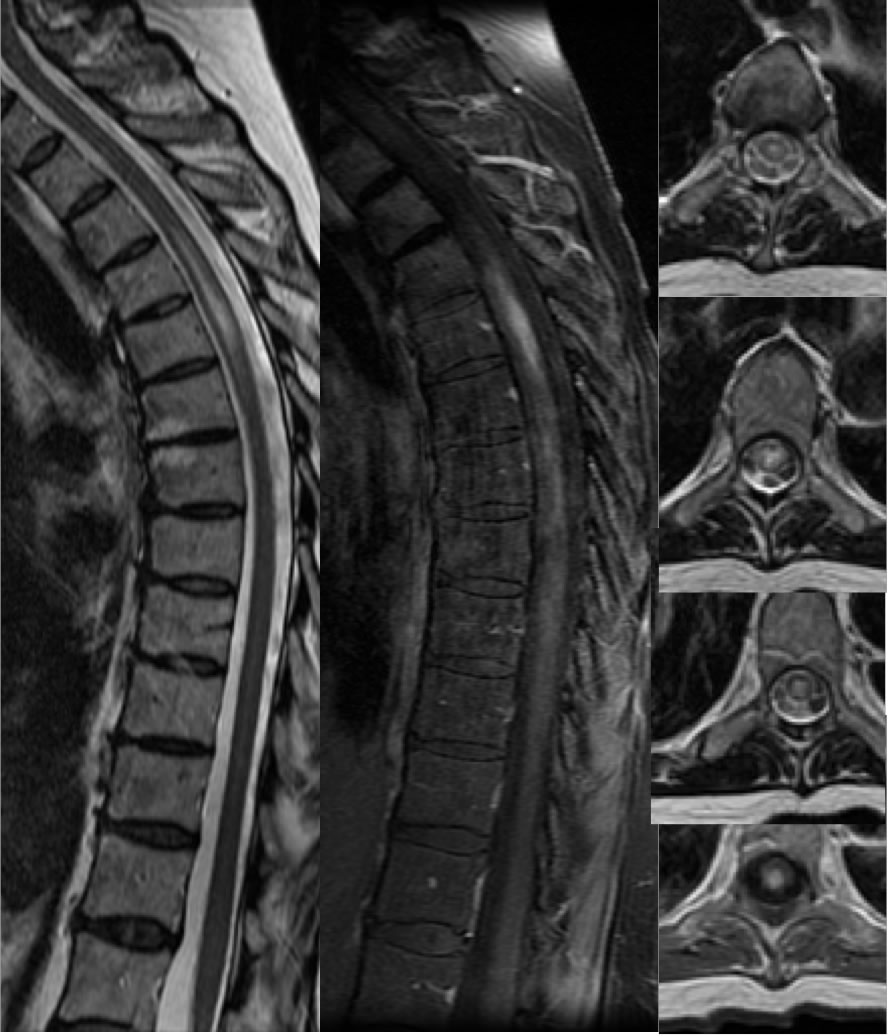
Sagittal T2, sagittal T1 post contrast with fat saturation, axial T2, and axial T1 post contrast images demonstrate a long segment of midline dorsal and central cord signal abnormality with dorsal patchy enhancement. There is subtle associated cord expansion. The process involves approximately three vertebral segments. Discogenic fatty endplate conversion is incidentally noted at a mid thoracic level.
Discussion/Differential Diagnosis:
The differential diagnosis for spinal cord signal abnormality is broad, including but not limited to MS and MS like processes including NMO, transverse myelitis of other cause, neoplasm, infarct, trauma, and compressive myelopathy. This process is less expansile than would be expected for neoplasm, involves a longer cord segment than would be expected for MS, and would not represent compressive myelopathy in the absence of cord compression or significant disc pathology. The location and morhology are not typical for infarct but not excluded. A long segment cord lesion with patchy enhancement and little or no cord expansion should raise suspicion for NMO.
NMO was previously known as Devic's disease as an inflammatory demyelinating process involving the spinal cord and optic nerves. NMO spectrum disorder (NMOSD) has a more variable range of abnormalities and probably is a more accurate designation. Autoantibodies to aquaporin 4 water channels are the apparent cause. Compared with MS, NMO may be seen in an older age group and with a stronger female predominance. It has a relapsing remitting course like MS, but episodes may be more widely spaced. The imaging features have some overlap with MS, but several distiguishers exist. These include longitudinally extensive spinal cord disease with grey matter involvement, central midline distribution (extensive corpus callosum involvement, diencephalon, brainstem), and longer segment of optic nerve involvement with swelling extending into chiasm. Characteristic Dawson's fingers are not seen. Similar to MS, ovoid and tumefactive hemispheric lesions may be seen. NMO is treated with immunosuppressives rather than immunomodulators which may exacerbate the course, therefore it is critical to establish the diagnosis by detecting aquaporin 4 IgG autoantibodies and not assume it is MS. (condensed from St-Amant and Gaillard, Radiopaedia)
-example of NMO with characteristic intracranial findings
BACK TO
MAIN PAGE