Heterotopic Gray Matter
Findings:
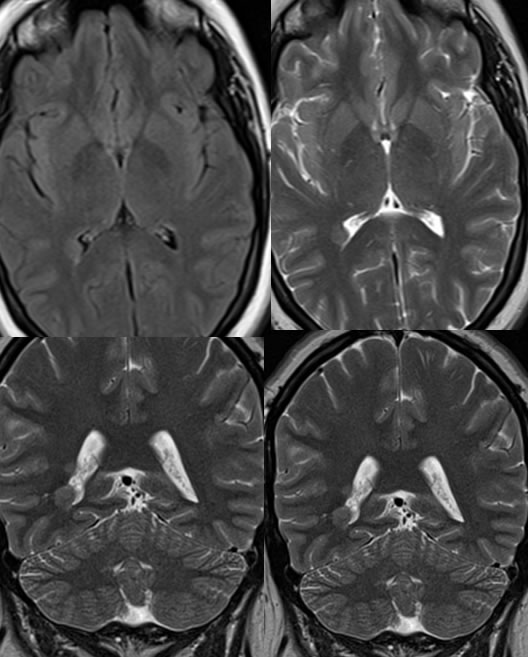
There is a focus of brain parenchyma following cortical signal extending from the rightperiatrial region along the lateral aspect of the right temporal horn to the posterior lateral margin of the right hippocampus, consistent with heterotopic gray matter. There is an additional discrete focus along the more superior lateral periatrial region of the right lateral ventricle.
Discussion/Differential Diagnosis:
A nodular subependymal signal abnormality has a differential diagnosis that includes primary or metastatic neoplasm, while ovoid periventricular white matter lesions without mass effect are more commonly related to demyelinating process. In this case, the distinguishing feature for heterotopic grey matter (HGM) is that the lesion is isointense to grey matter on all sequences. While postcontrast images are not shown, these lesions demonstrate no abnormal enhancement. If subependymal or subcortical nodules are calcified, TORCH infection or Tuberous Sclerosis could be considered since HGM very rarely calcifies. HGM is considered a migrational anomaly with arrested or disordered developmental migration of neurons that form in the subependymal germinal zones and travel along radial glial fibers to their final peripheral cortical location. This can be inherited or acquired. Subependymal nodules are most common, but there is a continuum to more extensive heterotopia including band morphology and lissencephaly. Clinical sequelae such as seizures and developmental delay tend to follow the extent of heterotopia, with small nodules often asymptomatic. HGM may be syndromic as with Chiari II, callosal agenesis, and X-linked disorders. HGM may also be acquired in CMV infection, fetal alcohol syndrome, or radiation exposure. The treatment focuses on medical seizure control, with surgery only for intractable seizures including removal of the focus or callosotomy for severe cases.
BACK TO
MAIN PAGE