Craniopharyngioma
Findings:
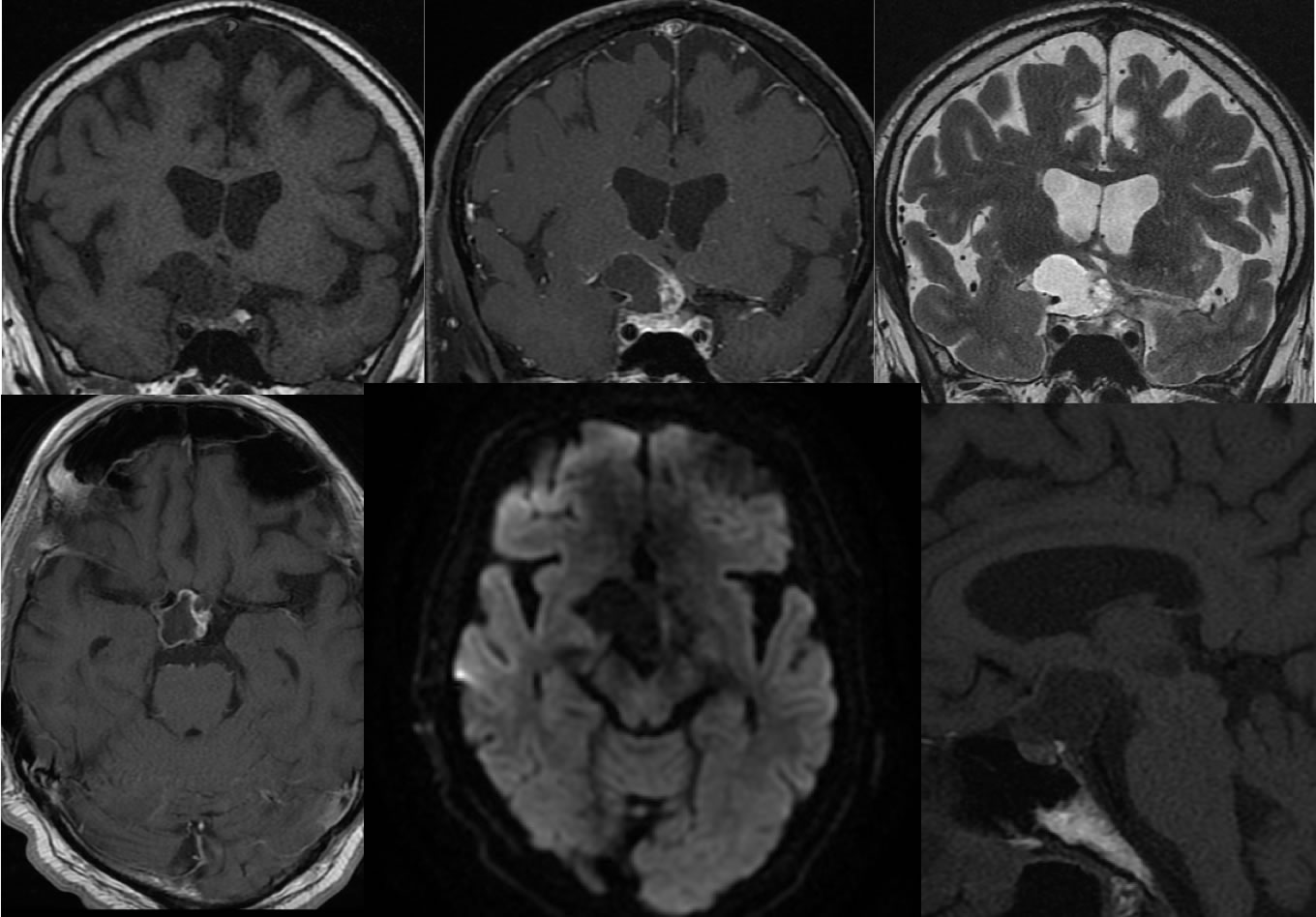
Multiple MR images demonstrate a complex cystic and solid suprasellar mass with irregular margins inseparable from the optic chiasm, pituitary infundibulum, and the right carotid terminus. The mass is separate from the pituitary gland. It does not demonstrate restricted diffusion.
Discussion/Differential Diagnosis:
The differential diagnosis of a sellar region mass may be narrowed by precise documention of the site of origin. A complex cystic and solid suprasellar mass that is clearly separate from the pituitary gland and also does not arise from the hypothalmus has the primary differential diagnosis of craniopharyngioma and teratoma. Dermoid/teratoma would be expected to have fat content and no nodular enhancement (not absolute). The adamaninomatous type is more common and seen in the pediatric population, while papillary types are seen in adults. Mixed types have similar prognosis to the adamantinomatous. These aere considered WHO grade 1 lesions, but may be locally invasive and difficult to resect with a risk for recurrence. The histology is not readily distiguishable from ameloblastoma of the mandible. Most are both supresellar and intrasellar components (75%) and less than 5% are purely intrasellar. 20% are purely suprasellar. Additional cases and discussion:
BACK TO
MAIN PAGE