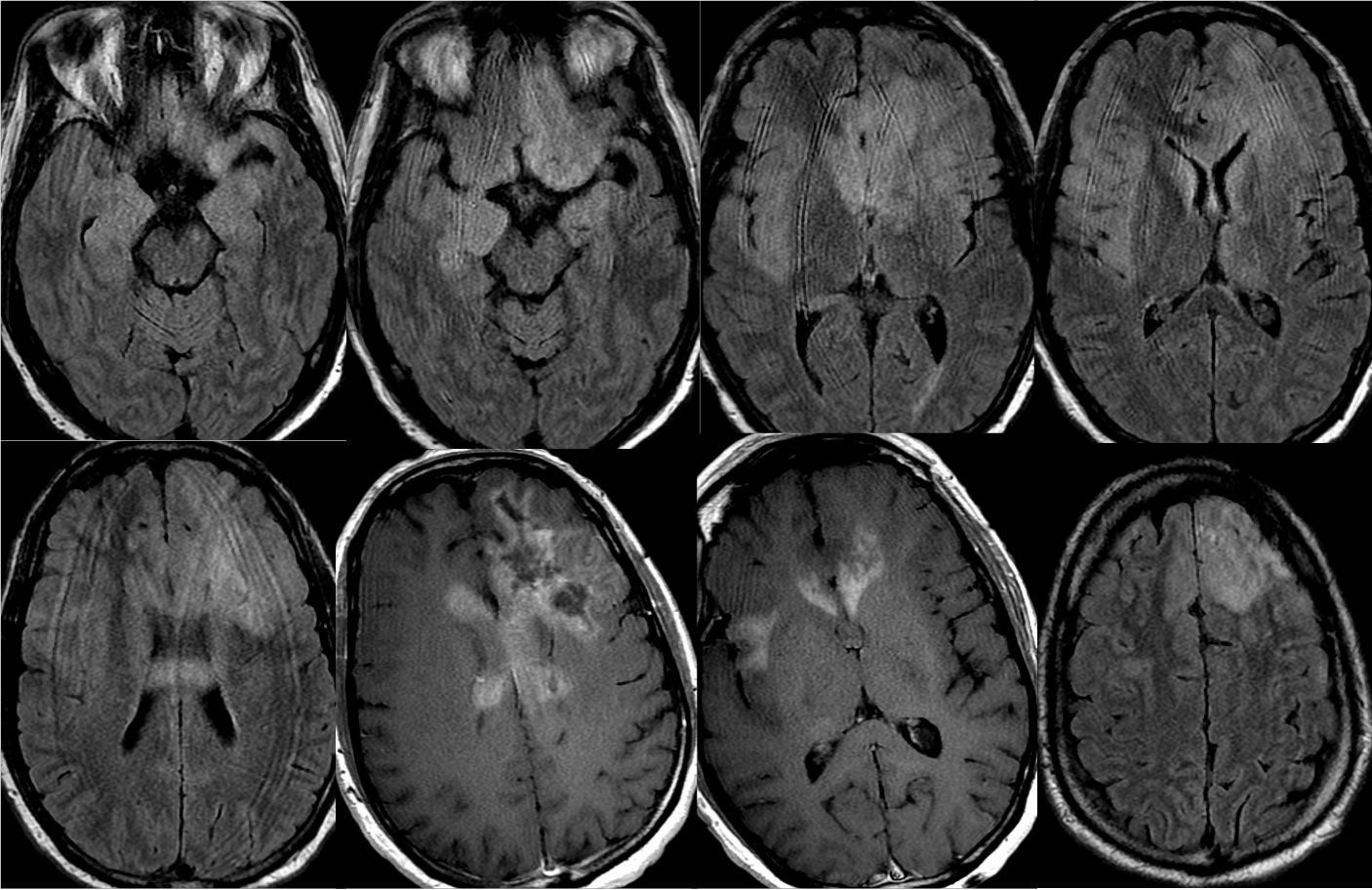
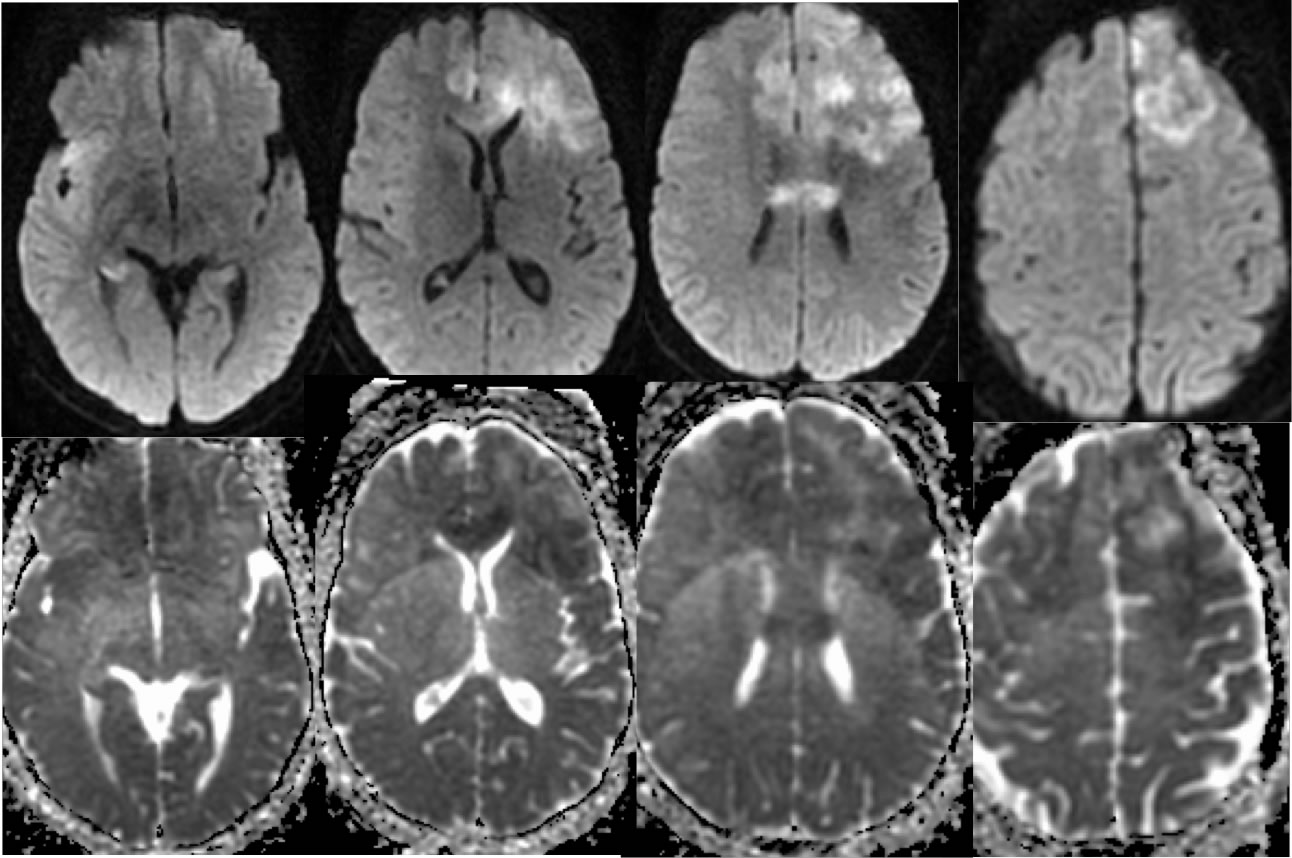
Gliomatosis Cerebri
Findings:
Axial FLAIR and T1 post contrast images demonstrate widespread confluent signal abnormalities involving the bilateral frontal lobes, temporal lobes, insula, and corpus callosum. Additional infiltrative signal abnormalities involve the bilateral caudate nuclei and left thalamus. Multifocal areas of gyral swelling are present. Numerous patchy zones of abnormal enhancement are present in this process, with some necrotic zones in the left frontal lobe. Mixed diffusion signal is present in these regions, with some areas of true restricted diffusion seen on the ADC map.
Discussion/Differential Diagnosis:
Gliomatosis cerebri (GC) is typically considered when there is infiltrative glial neoplastic involvement of at least 3 brain lobes. The prognosis is poor regradless of treatment. Clinical symptoms are nonspecific and may underestimate the disease burden. The 2016 WHO classification no longer recognizes GC as a discrete entity, but more as a growth pattern seen with many discrete types of infiltrative glioma. Additional discussion of GC and other primary glial malignancy:
-GBM
-GBM corpus callosum
-GBM w subependymal
-GBM intraventricular recurrence
-GBM spine w CSF dissemination
-recurrent GBM w uncal herniation
-recurrent GBM, corpus callosum
-GBM left frontal
-glioma/gliomatosis
cerebri
-gliomatosis
cerebri
-multifocal GBM
-GBM recurrence, dissemination
-GBM well circumscribed
-GBM recurrence, with dural sinus thrombosis
BACK TO
MAIN PAGE